

Comparative study of computed tomography of normal and lymphoid follicular hyperplasia thymus in myasthenia gravis patients
- PMID: 30651830
- PMCID: PMC6307392
- DOI: 10.3892/etm.2018.6948
Comparative study of computed tomography of normal and lymphoid follicular hyperplasia thymus in myasthenia gravis patients
Abstract
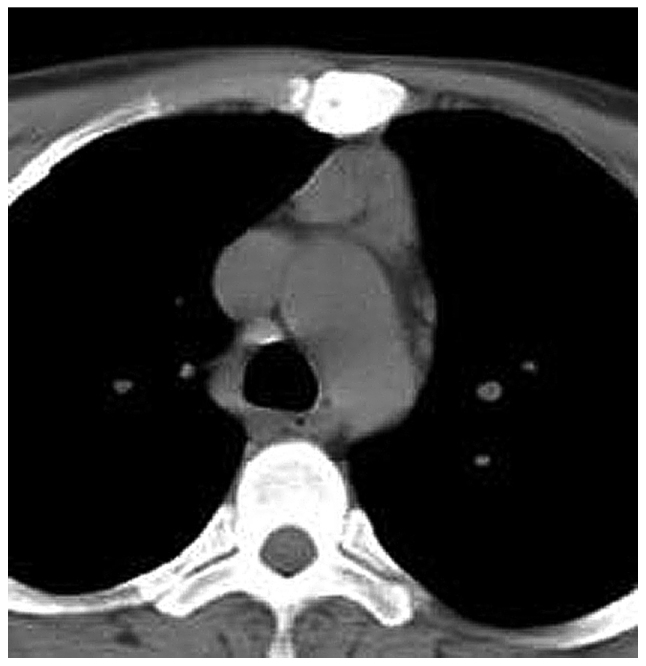
The aim of the present study was to evaluate the thymuses of non-thymomatous myasthenia gravis (MG) patients by computed tomography (CT) for differentiating lymphoid follicular hyperplasia (LFH) thymus from normal/involuted thymus in order to assist surgeons in determining whether a non-thymomatous MG patient requires an operation. In the present retrospective review over 10 years, 80 patients who received CT scan and thymectomy at the Affiliated General Hospital of Tianjin Medial University (Tianjin, China) were included. According to the pathological records, 54 of the cases initially detected on CT were confirmed as LFH thymus. Thymic measurements, including anteroposterior and transverse dimensions, width (the longest axis of the lobe on a transverse scan) and thickness (the largest dimension perpendicular to the long axis of the lobe) and CT attenuation of the thymus region, adipose tissue and chest wall musculature in each CT slice were included to assess differences between the LFH group and the normal/involuted thymus group. Although a negative association between patient age and the CT attenuation of the thymus region was identified (r=-0.779, P<0.05, Pearson's correlation test), the LFH thymus group featured nodular changes on CT, while no such changes were observed in the normal/involuted thymus group. The mean age of disease onset in the LFH thymus group was significantly lower than that in the normal thymus group (40.2±17.3 vs. 59.2±9.3 years). Furthermore, significant differences in CT attenuation were identified between the LFH group and the normal/involuted thymus group [-41.21±54.42 vs. -108.23±8.72 Hounsfield units (HU) on unenhanced CT; -25.57±58.65 vs.-117.40±6.22 HU on contrast-enhanced CT]. In the LFH group, the difference in mean CT attenuation between the thymus region and adipose tissue was significant, while no significant difference was observed in the normal/involuted thymus group. In conclusion, CT may be used to distinguish LFH thymus from normal/involuted thymus in MG patients.
Keywords: computed tomography; involuted thymus; lymphoid follicular hyperplasia; myasthenia gravis; thymectomy; thymus gland.
Figures











Similar articles
-
Thymic lesions in patients with myasthenia gravis: characterization with thallium 201 scintigraphy.Radiology. 2001 Oct;221(1):201-6. doi: 10.1148/radiol.2211001047. Radiology. 2001. PMID: 11568341
-
Comparative study of pre-operative thymic imaging and pathology in patients with myasthenia gravis.J Clin Neurosci. 2004 Aug;11(6):610-3. doi: 10.1016/j.jocn.2003.10.023. J Clin Neurosci. 2004. PMID: 15261231
-
Thymus in myasthenia gravis: comparison of CT and pathologic findings and clinical outcome after thymectomy.Radiology. 1996 Nov;201(2):471-4. doi: 10.1148/radiology.201.2.8888243. Radiology. 1996. PMID: 8888243
-
The role of humoral and cellular immune factors in neuromuscular block in myasthenia gravis.Ann N Y Acad Sci. 1976;274:493-515. doi: 10.1111/j.1749-6632.1976.tb47710.x. Ann N Y Acad Sci. 1976. PMID: 786115 Review.
-
Imaging of thymus in myasthenia gravis: from thymic hyperplasia to thymic tumor.Clin Radiol. 2014 May;69(5):e230-45. doi: 10.1016/j.crad.2014.01.005. Epub 2014 Feb 26. Clin Radiol. 2014. PMID: 24581970 Review.
Cited by
-
MASSIVE THYMIC HYPERPLASIA SECONDARY TO GRAVES DISEASE.AACE Clin Case Rep. 2020 May 8;6(3):e144-e146. doi: 10.4158/ACCR-2019-0423. eCollection 2020 May-Jun. AACE Clin Case Rep. 2020. PMID: 32524030 Free PMC article.
References
-
- Truffault F, de Montreville V, Eymard B, Sharshar T, Le Panse R, Berrih-Aknin S. Thymic germinal centers and corticosteroids in myasthenia gravis: An immunopathological study in 1035 cases and a critical review. Clin Rev Allergy Immunol. 2017;52:108–124. doi: 10.1007/s12016-016-8558-3. - DOI - PubMed
LinkOut - more resources
Full Text Sources