

Acquired hemophilia A presenting as progressive intra-abdominal hemorrhage, muscle hemorrhage and hemothorax postpartum: A case report and literature review
- PMID: 30651844
- PMCID: PMC6307365
- DOI: 10.3892/etm.2018.7031
Acquired hemophilia A presenting as progressive intra-abdominal hemorrhage, muscle hemorrhage and hemothorax postpartum: A case report and literature review
Abstract
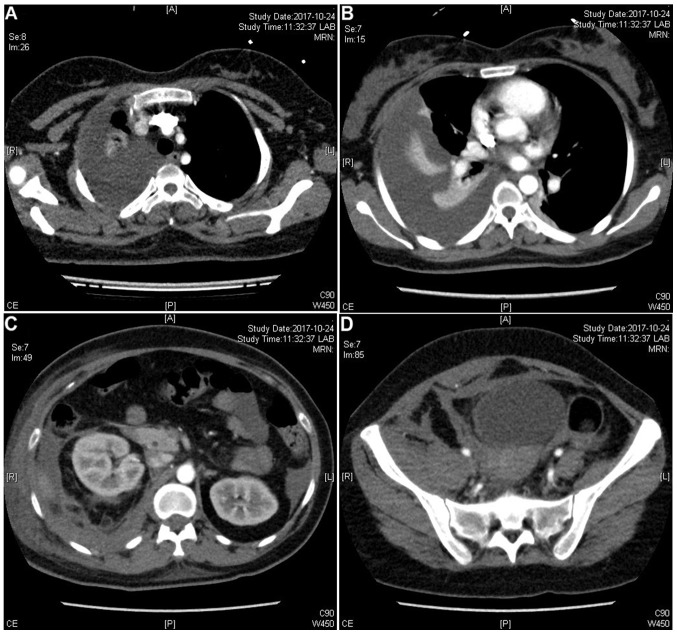
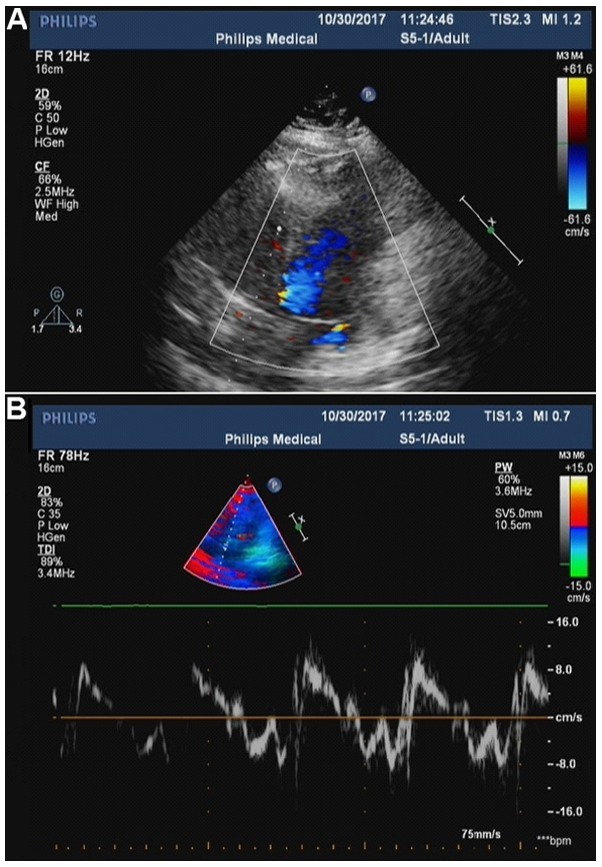
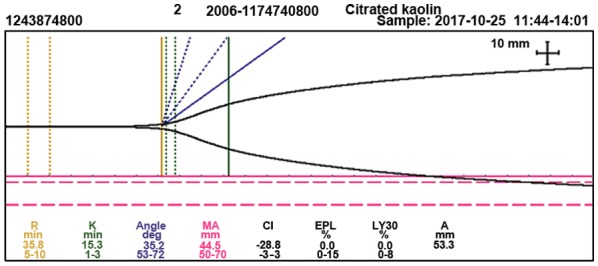
Acquired hemophilia A (AHA) is a rare antibody-mediated condition in which autoantibodies form against a coagulation factor, most commonly factor VIII (FVIII), causing severe coagulopathy. Here the present report presents a case of AHA in a 35-year-old postpartum woman with continuous polyserous bloody effusions who was admitted to the First Affiliated Hospital of Zhejiang Chinese Medical University (Hangzhou, China) in October 2017 without a history of trauma, anticoagulation treatment or coagulopathy. At presentation, the patient's hemoglobin level was low (70 g/l; normal range: 115-150 g/l) g/l, blood pressure was 89/58 mmHg (normal range, 90-140/60-90 mmHg), and activated partial thromboplastin time was 68.4 sec (normal range: 25.0-36.0 sec), with a normal international normalized ratio (0.94; normal range, 0.8-1.2). The reaction time in thrombography was prolonged (35.8 min; normal range: 5-10 min), coagulation FVIII had markedly decreased activity (12.6%; normal range, 60-150%), and FVIII inhibitor had a high titer [7.4 Bethesda units (BU)/ml; normal range, 0-0.6 BU/ml]. Notably, the patient's autoantibody level was markedly higher than normal (1:320; normal range: <1:100). The patient was successfully treated with bleeding control, eradication of FVIII inhibitor, and treatment of the underlying disease. To the best of our knowledge, this is the first case of AHA with polyserous bloody effusions in a patient with an autoimmune disorder during the postpartum period. Reports of such rare cases will aid the characterization of disease pathogenesis, which may in turn lead to the recognition and timely treatment of this rare disorder.
Keywords: China; acquired hemophilia A; hemorrhage; polyserous effusions; premature delivery.
Figures
Similar articles
-
The first case of postpartum acquired hemophilia A in Korea.J Korean Med Sci. 2011 Sep;26(9):1247-9. doi: 10.3346/jkms.2011.26.9.1247. Epub 2011 Sep 1. J Korean Med Sci. 2011. PMID: 21935285 Free PMC article.
-
[Systemic lupus erythematosus with acquired hemophilia A: a case report].Beijing Da Xue Xue Bao Yi Xue Ban. 2018 Dec 18;50(6):1108-1111. Beijing Da Xue Xue Bao Yi Xue Ban. 2018. PMID: 30562791 Chinese.
-
Combined life-threatening internal organ bleeding and postpartum hemorrhage associated with acquired hemophilia A.Clin Case Rep. 2024 Jan 2;12(1):e8399. doi: 10.1002/ccr3.8399. eCollection 2024 Jan. Clin Case Rep. 2024. PMID: 38173887 Free PMC article.
-
Acquired inhibitors of coagulation factors: part I-acquired hemophilia A.Semin Thromb Hemost. 2012 Jul;38(5):433-46. doi: 10.1055/s-0032-1315757. Epub 2012 Jun 27. Semin Thromb Hemost. 2012. PMID: 22740182 Review.
-
Acquired hemophilia A secondary to cholangiocarcinoma: A case report and literature review.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2025 Feb 28;50(2):275-280. doi: 10.11817/j.issn.1672-7347.2025.240037. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2025. PMID: 40523770 Review. Chinese, English.
Cited by
-
Acquired factor VIII deficiency in a nulliparous patient undergoing induction of labor.Case Rep Perinat Med. 2024 Mar 11;13(1):20230004. doi: 10.1515/crpm-2023-0004. eCollection 2024 Jan. Case Rep Perinat Med. 2024. PMID: 40321343 Free PMC article.
-
Recognition of the unique bleeding pattern and laboratory findings in acquired haemophilia A facilitates prompt treatment of a life-threatening disorder.BMJ Case Rep. 2021 Aug 3;14(8):e244238. doi: 10.1136/bcr-2021-244238. BMJ Case Rep. 2021. PMID: 34344656 Free PMC article.
-
A Rare Case of Acquired Factor VIII Deficiency in an Elderly Male With a History of Rheumatoid Arthritis.Cureus. 2023 Aug 26;15(8):e44169. doi: 10.7759/cureus.44169. eCollection 2023 Aug. Cureus. 2023. PMID: 37753049 Free PMC article.
References
-
- Vautier M, de Boysson H, Creveuil C, Repesse Y, Borel-Derlon A, Troussard X, Damaj GL, Bienvenu B, Gautier P, Aouba A. Influence of factor VIII level and its inhibitor titer on the therapeutic response to corticosteroids alone in the management of acquired hemophilia. Medicine (Baltimore) 2016;95:e5232. doi: 10.1097/MD.0000000000005232. - DOI - PMC - PubMed
-
- Olteanu M, Niţu M, Golli A. Tuberculosis mesenteric adenopathy and polyserositis. Rom J Morphol Embryol. 2012;53:835–840. - PubMed
LinkOut - more resources
Full Text Sources