

Clinical observation of orbital IgG4-related diseases
- PMID: 30651876
- PMCID: PMC6307391
- DOI: 10.3892/etm.2018.7002
Clinical observation of orbital IgG4-related diseases
Abstract
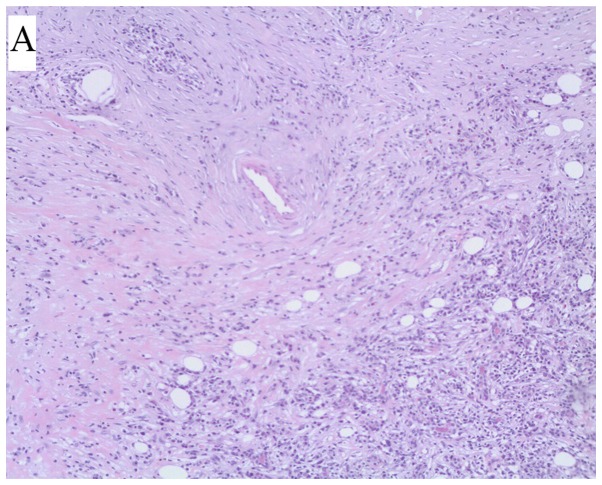
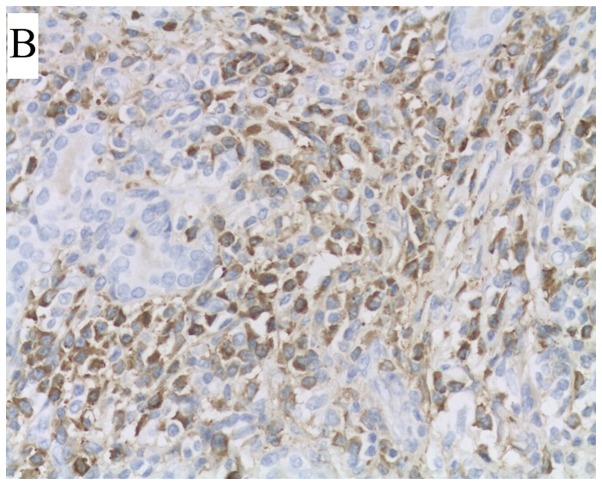
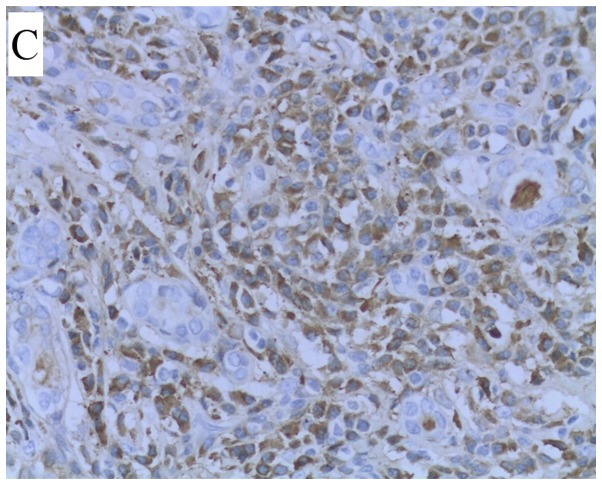
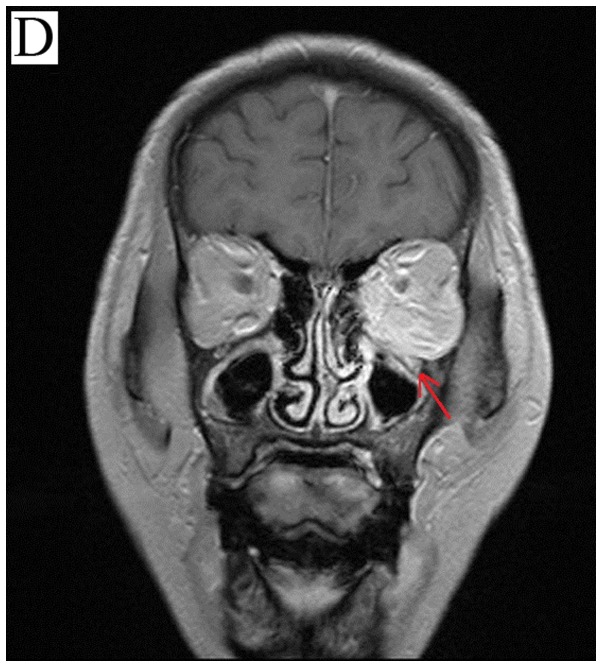
The aim of the present study was to observe the histopathological changes of immunoglobulin G4-related orbital diseases (IgG4-RODs), summarize the clinical manifestations and imaging features of the IgG4-RODs of the eyelids and explore the early diagnosis of IgG4-RODs. Between June 2011 and May 2015, 23 patients with non-specific orbital inflammation in the Department of Ophthalmology at the First Central Hospital of Tianjin were recruited. The serum IgG4 titer in 9 patients ranged from 4.58 to 46.70 g/l (reference value, 0.03-2.01 g/l), with an average value of 21.93±2.18 g/l. Notably, the degree of increase in the 9 patients with IgG4-RODs was different, but all were >1.35 g/l. A total of 6 cases of infraorbital nerve thickening were observed. In addition, there were 3 cases of extraocular muscle thickening and 1 patient with IgG4-ROD had an orbital tissue lesion extending along the inferior temporal septum to the left pterygopalatine fossa, with left sacral fissure widening and involvement of the left maxillary sinus. The study revealed that the thickening of the inferior orbital nerve may be a characteristic of IgG4-ROD. Therefore, on the basis of biopsy and serological examination in the clinic, early diagnosis can be combined with imaging examination, clinical manifestation and laboratory examination, so as to reduce misdiagnosis and missed diagnosis.
Keywords: IgG4-related eye disease; differential diagnosis; immunoglobulin G; immunohistochemistry; orbital disease.
Figures
References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases