

Imaging features of uterine and ovarian fibromatosis in Nevoid Basal Cell Carcinoma Syndrome
- PMID: 30651920
- PMCID: PMC6312044
- DOI: 10.3941/jrcr.v12i9.3390
Imaging features of uterine and ovarian fibromatosis in Nevoid Basal Cell Carcinoma Syndrome
Abstract
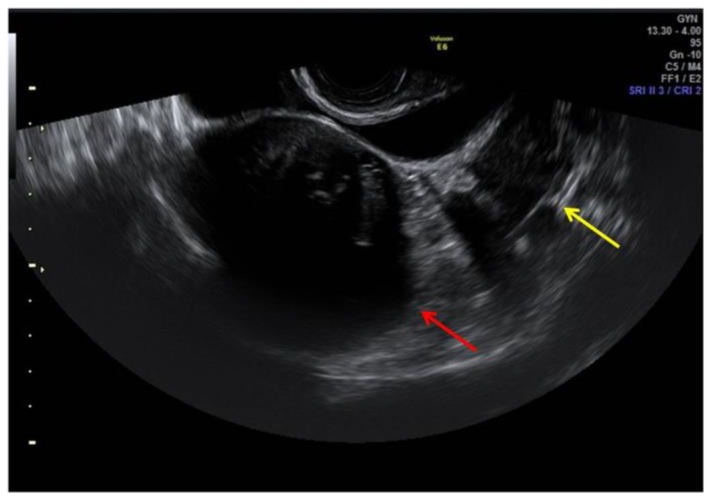
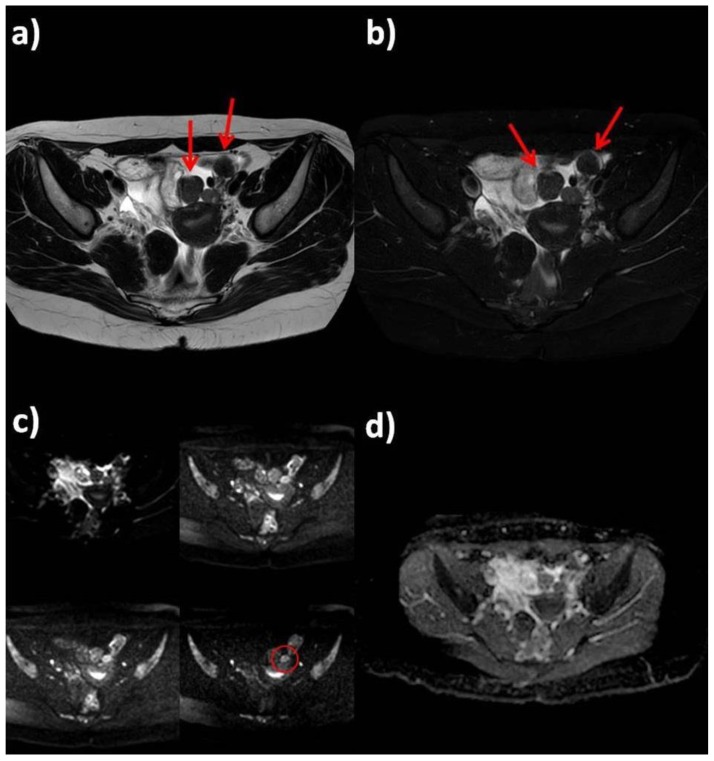
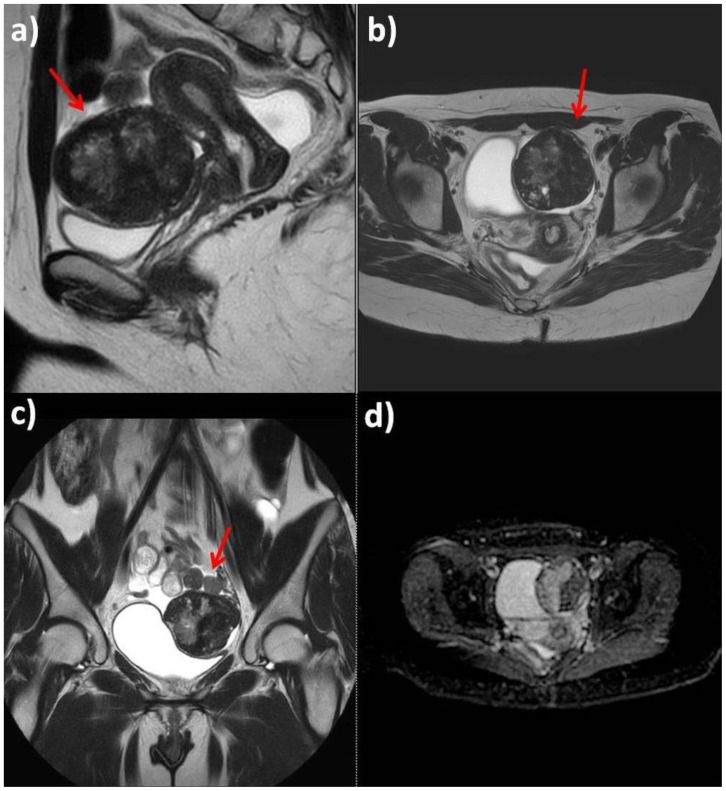
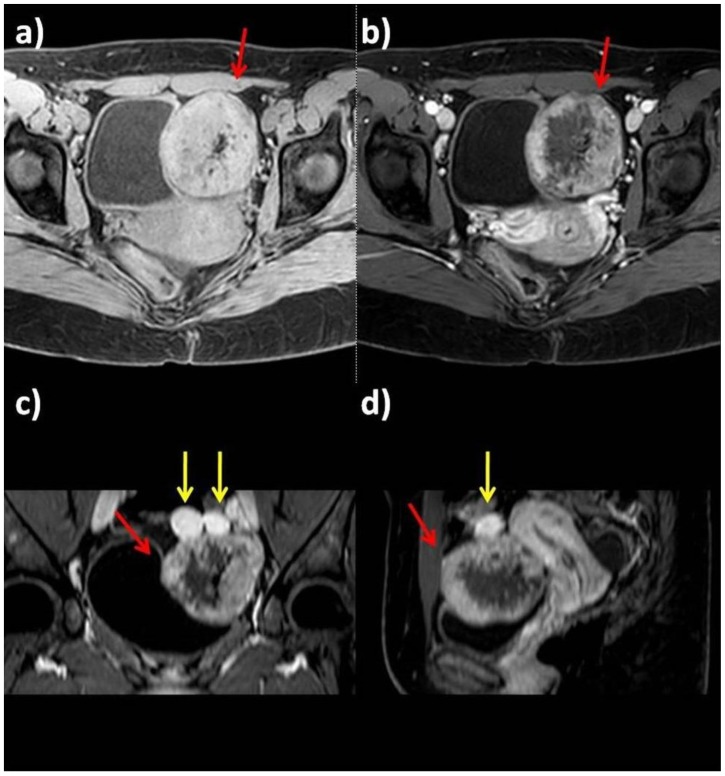
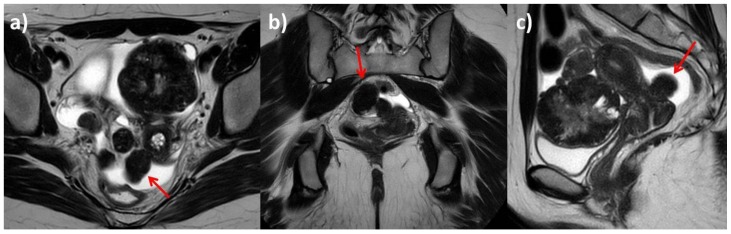
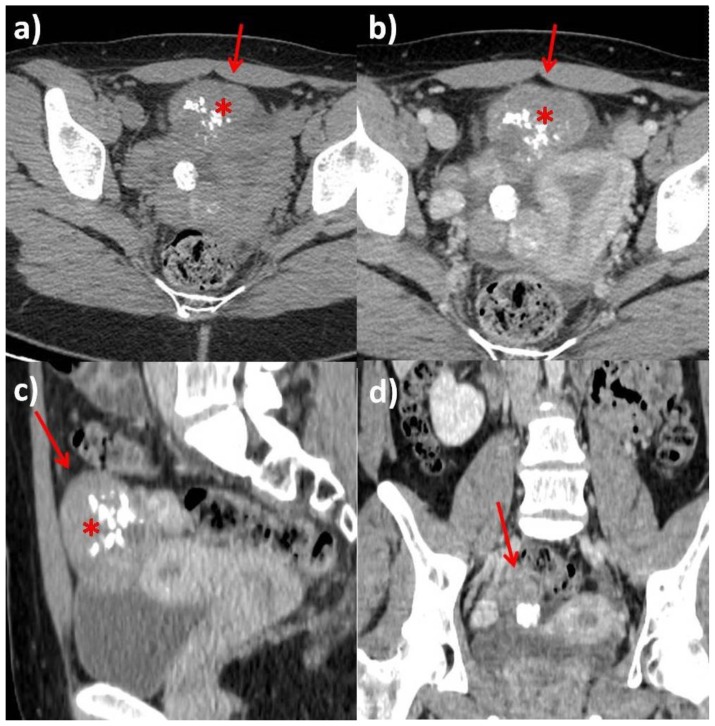
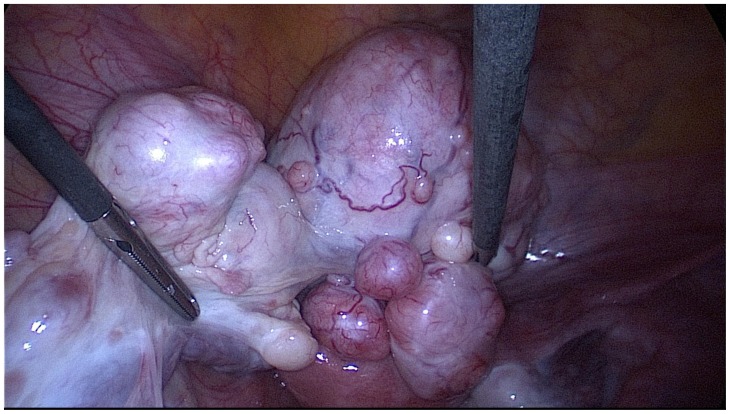
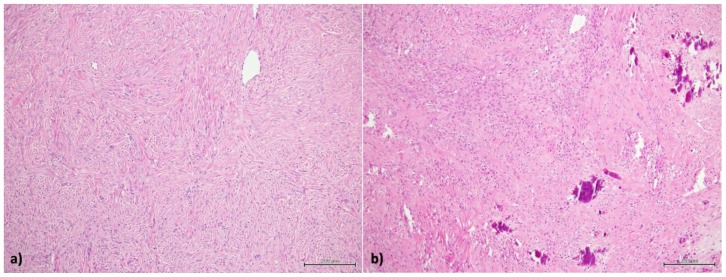
Gorlin-Goltz Syndrome also known as Nevoid Basal Cell Carcinoma Syndrome is an autosomal dominant multisystem disorder. It is characterized by basal cell carcinomas, odontogenic keratocysts, skeletal abnormalities and in a minority of female patients bilateral calcified ovarian fibromas. It is challenging to radiologically assess ovarian fibromas as they have similar imaging patterns to some malignant ovarian lesions. However, it is vitally important to differentiate between benign and malignant lesions to determine patients' suitability for fertility-sparing surgery. This report describes a case of a 25 year-old patient with Gorlin-Goltz Syndrome and bilateral ovarian fibromas.
Keywords: Gorlin-Goltz syndrome; MRI; NBCCS; ovarian fibromas; uterine fibromas.
Figures
References
-
- Evans DG, Farndon PA. Nevoid Basal Cell Carcinoma Syndrome. GeneReviews® 2018. 2002. Jun 20, [Updated 2018 Mar 29]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK1151/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical