

Association between lymphocyte count and neurological outcomes in post-cardiac arrest patients treated with mild therapeutic hypothermia
- PMID: 30651995
- PMCID: PMC6328908
- DOI: 10.1002/ams2.374
Association between lymphocyte count and neurological outcomes in post-cardiac arrest patients treated with mild therapeutic hypothermia
Abstract
Aim: To examine lymphocyte counts as a predictive prognostic marker in patients with coma after cardiac arrest.
Methods: We retrospectively evaluated patients with coma after cardiac arrest admitted to the intensive care unit of Shiga University of Medical Science (Otsu, Japan). Lymphocyte counts were measured for 6 days from admission. Neurological outcome was assessed as favorable or unfavorable using cerebral performance categories. Associations between lymphocyte count and prognosis were investigated using multivariate logistic regression analysis and receiver operating characteristic curves.
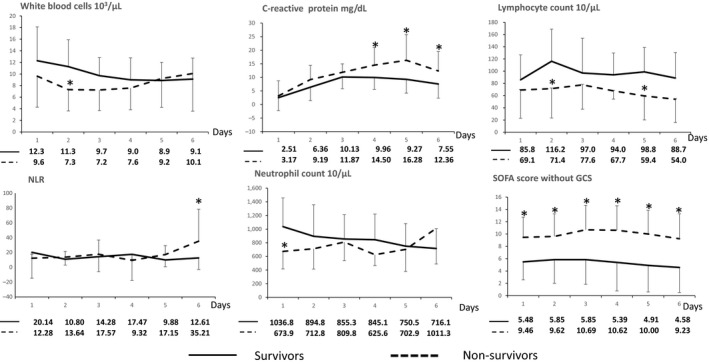
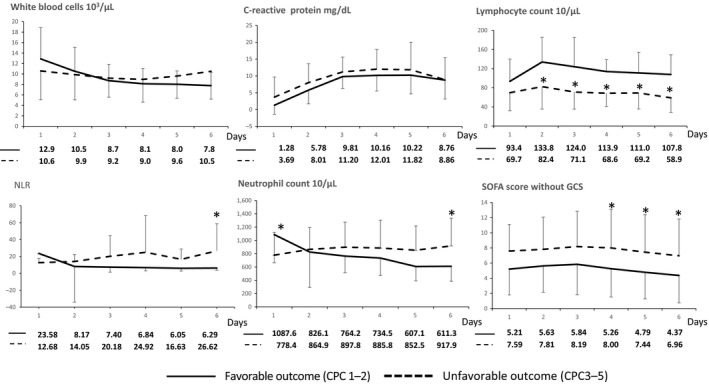
Results: Forty-six patients were assessed from February 2012 to December 2016. Survivors had significantly higher lymphocyte counts than non-survivors on days 2 and 5. Multivariate analysis showed that lymphocyte count was not associated with 90-day mortality. Patients with favorable neurological outcome at discharge had significantly higher lymphocyte counts on days 2-6 than patients with unfavorable outcomes. Multivariate logistic regression analysis, including possible confounders, showed that lymphocyte counts on days 2-4 and 6 were associated with neurological outcome (day 2: odds ratio [OR] = 0.75, 95% confidence interval [CI] = 0.58-0.97, P = 0.029; day 3: OR = 0.68, 95% CI = 0.47-0.98, P = 0.04; day 4: OR = 0.4, 95% CI = 0.16-1.00, P = 0.05; day 6: OR = 0.69, 95% CI = 0.48-0.99, P = 0.046). Receiver operating characteristic curve analysis indicated high accuracy for predicting neurological outcome for each lymphocyte count on days 2-6 using the area under the curve, day 4 values being most accurate (day 2: 0.776, day 3: 0.787, day 4: 0.909, day 5: 0.774, day 6: 0.839).
Conclusion: Lymphocyte counts on days 2-4 and 6 after cardiac arrest are associated with neurological outcome; counts on day 4 most accurately predict neurological outcome.
Keywords: Cardiopulmonary arrest; lymphocyte; lymphopenia; prognosis; therapeutic hypothermia.
Figures
References
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out‐of‐hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation 2010; 81: 1479–87. - PubMed
-
- Nolan JP, Neumar RW, Adrie C et al Post‐cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008; 118: 2452–83. - PubMed
-
- Weiser C, Schwameis M, Sterz F et al Mortality in patients resuscitated from out‐of‐hospital cardiac arrest based on automated blood cell count and neutrophil lymphocyte ratio at admission. Resuscitation 2017; 116: 49–55. - PubMed
LinkOut - more resources
Full Text Sources
