

Voice outcome after unilateral ELS type III or bilateral type II resections for T1-T2 glottic carcinoma: Results after 1 year
- PMID: 30652373
- PMCID: PMC6590407
- DOI: 10.1002/hed.25582
Voice outcome after unilateral ELS type III or bilateral type II resections for T1-T2 glottic carcinoma: Results after 1 year
Abstract
Background: Voice outcome was assessed in patients with extended T1 and limited T2 glottic carcinoma, treated with a unilateral type III or a bilateral type II resection according to the European Laryngological Society (ELS) classification.
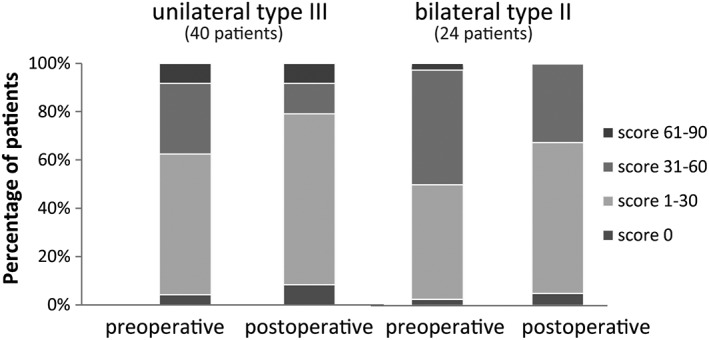
Methods: Objective evaluation (acoustic and aerodynamic parameters), perceptual evaluation (GRBAS), and patients' self-assessment (voice handicap index [VHI]) were performed before and 1 year after treatment. Results were evaluated according to ELS resection type and the involvement of the anterior commissure.
Results: The majority of voice parameters in all resection subgroups showed an improvement of the mean score 1 year postoperatively. Grade of dysphonia varied between 1.15 and 1.66 postoperatively and VHI score varied from 23.3 to 24.5.
Conclusion: Voice outcome after ELS unilateral type III or a bilateral type II resection for extended T1 and limited T2 glottic carcinoma is good with mild to very moderate perceptive dysphonia and low self-reported voice impairment.
Keywords: TLM; anterior commissure involvement; early glottic cancer; laser surgery; voice outcome.
© 2019 The Authors. Head & Neck published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Abdurehim Y, Hua Z, Yasin Y, Xukurhan A, Imam I, Yuqin F. Transoral laser surgery versus radiotherapy: systematic review and meta‐analysis for treatment options of T1a glottic cancer. Head Neck. 2012;34(1):23‐33. - PubMed
-
- Low THH, Yeh D, Zhang T, et al. Evaluating organ preservation outcome as treatment endpoint for T1aN0 glottic cancer. Laryngoscope. 2017;127(6):1322‐1327. - PubMed
-
- Mahler V, Boysen M, Brondbo K. Radiotherapy or CO(2) laser surgery as treatment of T(1a) glottic carcinoma? Eur Arch Otorhinolaryngol. 2010;267(5):743‐750. - PubMed
-
- Schrijvers ML, Van Riel EL, Langendijk JA, et al. Higher laryngeal preservation rate after CO2 laser surgery compared with radiotherapy in T1a glottic laryngeal carcinoma. Head Neck. 2009;31(6):759‐764. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
