

Slipped capital femoral epiphysis in an adult with congenital hypopituitarism: A case report
- PMID: 30653105
- PMCID: PMC6370171
- DOI: 10.1097/MD.0000000000013997
Slipped capital femoral epiphysis in an adult with congenital hypopituitarism: A case report
Abstract
Rationale: Slipped capital femoral epiphysis (SCFE) is a common hip problem in adolescents, usually individuals between 8 and 15 years old. Because of the frequent finding of growth abnormalities in affected children, various endocrine disturbances have been reported as the cause of the disease. However, there are few case reports of older patients in previous literature. To the best of our knowledge, congenital hypopituitarism with normal growth hormone (GH) level has not been reported.
Patient concerns: We describe a 29-year-old man who had a 3-month history of pain in the left hip with tall stature and unobvious secondary sexual characteristics. Laboratory testing showed low thyroxine, low cortisol, low follicle-stimulating hormone, low luteinizing hormone, low testosterone, but normal GH.
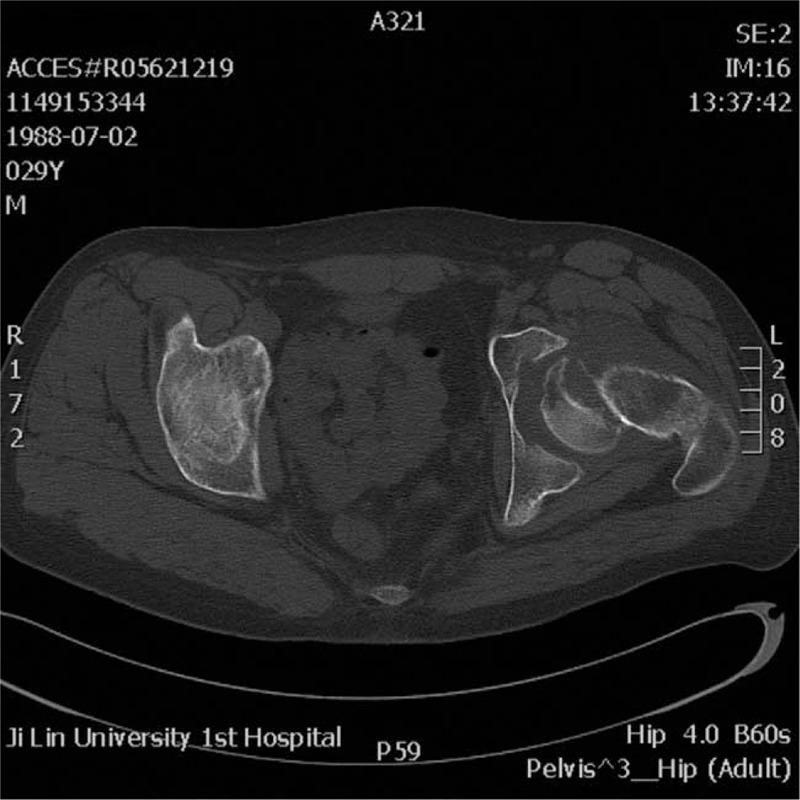
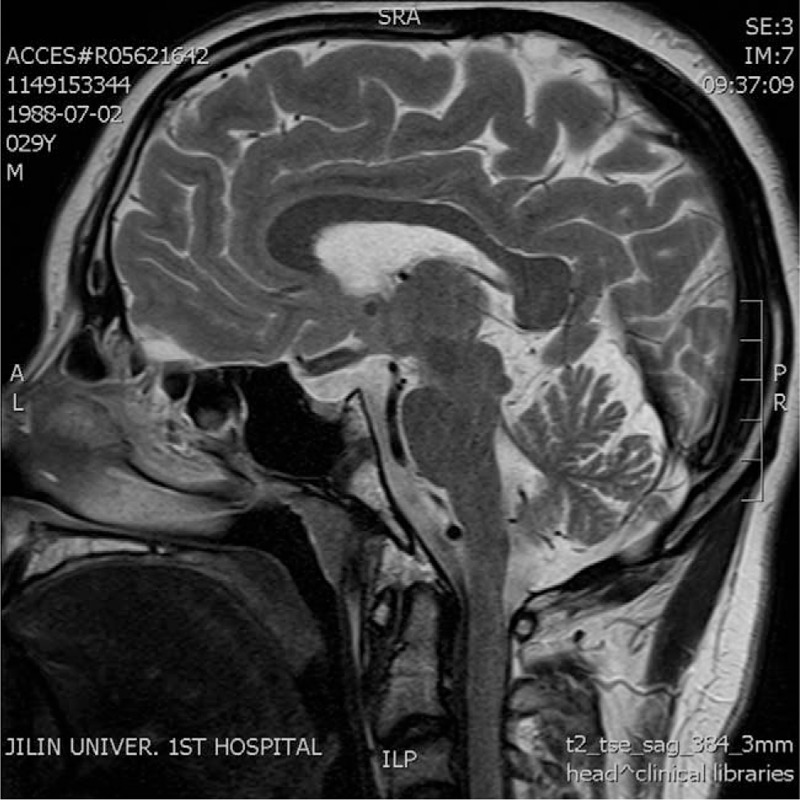
Diagnoses: Brain magnetic resonance imaging showed pituitary hypoplasia. An anteroposterior pelvis radiograph showed severe varus SCFE in the left hip, it was also confirmed with computed tomography scans.
Interventions: The patient was treated with levothyroxine, hydrocortisone, and testosterone replacement therapy before surgery. We performed open reduction and anatomical reduction by Dunn's procedure.
Outcome: We have followed this patient for 6 months, the left hip mobility gradually improved. No slip in the contralateral proximal femoral physis has been observed.
Lessons: When unobvious secondary sexual characteristics and body abnormalities were found in clinical practice, endocrine condition should be evaluated, since the contralateral side may prone to slip due to the lack of endocrine therapy.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures



Similar articles
-
Slipped capital femoral epiphysis with hypopituitarism in adults: A case report and literature review.Medicine (Baltimore). 2021 Dec 23;100(51):e28256. doi: 10.1097/MD.0000000000028256. Medicine (Baltimore). 2021. PMID: 34941101 Free PMC article. Review.
-
Morphologic Features of the Contralateral Femur in Patients With Unilateral Slipped Capital Femoral Epiphysis Resembles Mild Slip Deformity: A Matched Cohort Study.Clin Orthop Relat Res. 2018 Apr;476(4):890-899. doi: 10.1007/s11999.0000000000000127. Clin Orthop Relat Res. 2018. PMID: 29481345 Free PMC article.
-
Valgus slipped capital femoral epiphysis with contralateral pre-slip.Skeletal Radiol. 2017 Sep;46(9):1261-1265. doi: 10.1007/s00256-017-2654-1. Epub 2017 Apr 28. Skeletal Radiol. 2017. PMID: 28455719
-
The results of osteotomy at the base of femoral neck with osteoplasty in restoration of abductor function and strength in slipped capital femoral epiphysis.Bone Joint J. 2018 Nov;100-B(11):1524-1532. doi: 10.1302/0301-620X.100B11.BJJ-2018-0273.R1. Bone Joint J. 2018. PMID: 30418052
-
Surgical management of healed slipped capital femoral epiphysis.J Am Acad Orthop Surg. 2011 Nov;19(11):667-77. doi: 10.5435/00124635-201111000-00003. J Am Acad Orthop Surg. 2011. PMID: 22052643 Review.
Cited by
-
Primary Hypothyroidism Presenting as Slipped Capital Femoral Epiphysis in an Adult Patient : A Case Report and Review of Literature.J Orthop Case Rep. 2021 Nov;11(11):16-18. doi: 10.13107/jocr.2021.v11.i11.2496. J Orthop Case Rep. 2021. PMID: 35415117 Free PMC article.
-
Slipped Capital Femoral Epiphysis in an Adult Patient With Kabuki Syndrome.J Am Acad Orthop Surg Glob Res Rev. 2019 Oct 14;3(10):e19.00084. doi: 10.5435/JAAOSGlobal-D-19-00084. eCollection 2019 Oct. J Am Acad Orthop Surg Glob Res Rev. 2019. PMID: 31773073 Free PMC article.
-
Slipped Capital Femoral Epiphysis Managed by Ganz Safe Surgical Dislocation of Hip: A Case Report with 2 Years Follow-up.J Orthop Case Rep. 2022 Aug;12(8):38-41. doi: 10.13107/jocr.2022.v12.i08.2956. J Orthop Case Rep. 2022. PMID: 36687473 Free PMC article.
-
Epiphysiolysis in a 22-year-old Patient with Congenital Hypogonadotropic Hypogonadism: Case Report.Rev Bras Ortop (Sao Paulo). 2021 Apr 19;58(6):e960-e963. doi: 10.1055/s-0041-1726071. eCollection 2023 Dec. Rev Bras Ortop (Sao Paulo). 2021. PMID: 38077755 Free PMC article.
-
Slipped capital femoral epiphysis in an adolescent with congenital adrenal hyperplasia: A case report.Clin Case Rep. 2024 Jun 28;12(7):e9131. doi: 10.1002/ccr3.9131. eCollection 2024 Jul. Clin Case Rep. 2024. PMID: 38947535 Free PMC article.
References
-
- Song MH, Jang WY, Park MS, et al. Slipped capital femoral epiphysis in children younger than 10 years old: clinical characteristics and efficacy of physeal-sparing procedures. J Pediatr Orthop B 2018;27:379–86. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
