

Clinical and radiological outcomes of a cervical cage with integrated fixation
- PMID: 30653129
- PMCID: PMC6370175
- DOI: 10.1097/MD.0000000000014097
Clinical and radiological outcomes of a cervical cage with integrated fixation
Abstract
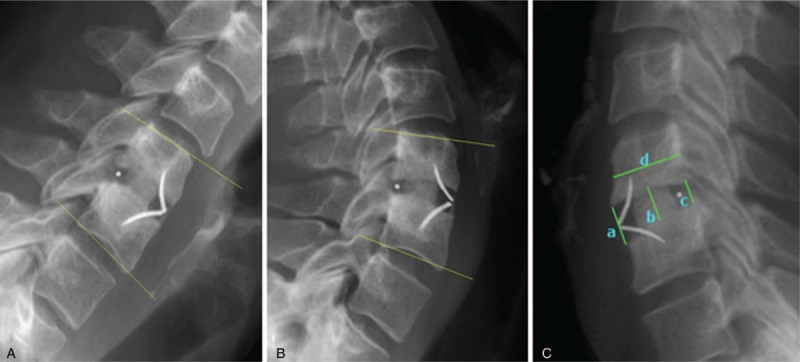
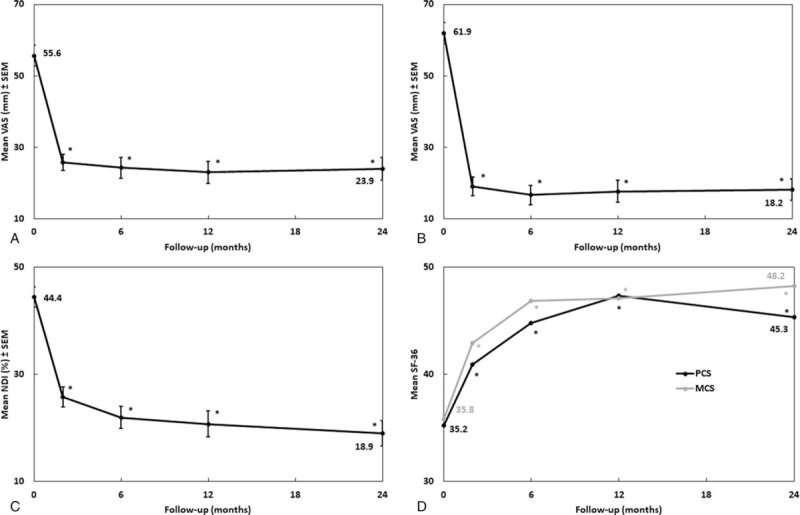
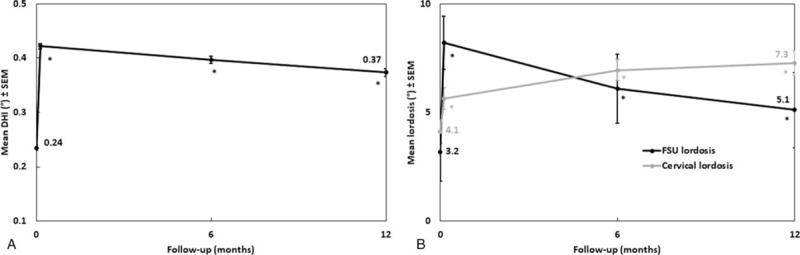
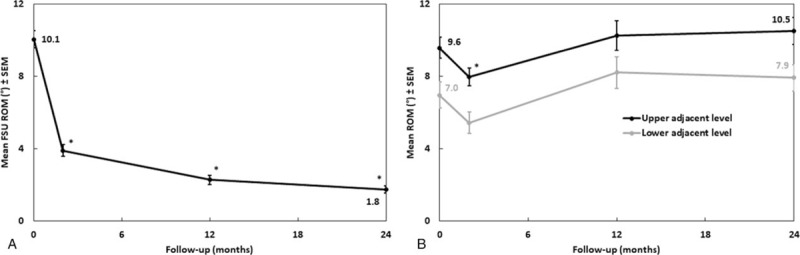
Cervical cages with integrated fixation have been increasingly used in anterior cervical discectomy and fusion (ACDF) to avoid complications associated with anterior cervical plates. The purpose of this paper is to provide 2-year follow-up results of a prospective study after implantation of a cervical cage with an integrated fixation system.This was a prospective multicenter outcome study of 90 patients who underwent ACDF with a cage with integrated fixation. Fusion was evaluated from computed tomography images (CT-images) by an independent laboratory at 2-year follow-up (FU). Clinical and radiological findings were recorded preoperatively and at FU visits and complications were reported.At 24 months, the fusion rate was 93.4%. All average clinical outcomes were significantly improved at 2 years FU compared to baseline: neck disability index (NDI) 18.9% vs 44.4%, visual analog scale (VAS) for arm pain 18.2 mm vs 61.9 mm, VAS for neck pain 23.9 mm vs 55.6 mm. Short form-36 (SF-36) scores were significantly improved. One case of dysphagia, which resolved within 12 months, and 1 reoperation for symptomatic pseudarthrosis were reported. Subsidence with no clinical consequence or reoperation was reported for 5/125 of the implanted cages (4%). There was also 1 case of per-operative vertebral body fracture that did not require additional surgery. Superior and inferior adjacent discs showed no significant change of motion at 2-year FU compared to baseline. Disc height index (DHI) and lordosis were enhanced and these improvements were maintained at 1 year.The ACDF using cages with an integrated fixation system demonstrated reliable clinical and radiological outcomes and a high interbody fusion rate. This rate is comparable to the rate reported in recent series using other implants with integrated fixation, but the present device had a lower complication rate.
Conflict of interest statement
The authors of this manuscript have the following competing interests: Jean Huppert reports royalties from Zimmer Biomet not relating to the submitted work. Manuel Delhaye reports royalties from Zimmer Biomet and Spine Art not relating to the submitted work, and consulting activities for Medtronic and Spine Art. Ramzi Mraidi is a Zimmer Biomer employee. Nicolas Lonjon, Emmanuel Favreul, and Eric Lioret report no competing interests.
Figures
References
-
- Jacobs W, Willems PC, Kruyt M, et al. Systematic review of anterior interbody fusion techniques for single- and double-level cervical degenerative disc disease. Spine 2011;36:E950–960. - PubMed
-
- Jacobs WC, Anderson PG, Limbeek J, et al. Single or double-level anterior interbody fusion techniques for cervical degenerative disc disease. Cochrane Database Syst Rev 2004;4:CD004958. - PubMed
-
- Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurosurg 1958;15:602–17. - PubMed
-
- Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40-A:607–24. - PubMed
-
- Anderson DG, Albert TJ. Bone grafting, implants, and plating options for anterior cervical fusions. Orthop Clin North Am 2002;33:317–28. - PubMed
