

Surgical management of spinal metastases of thymic carcinoma: A case report and literature review
- PMID: 30653174
- PMCID: PMC6370146
- DOI: 10.1097/MD.0000000000014198
Surgical management of spinal metastases of thymic carcinoma: A case report and literature review
Abstract
Rationale: Metastatic thymic carcinoma in the spine is a rare disease with no standard curative managements yet. The objective of this study is to report a very rare case of spinal metastases of thymic carcinoma successfully operated by combination of instrumentation and cement augmentation together with adjuvant treatment. The management of these unique cases has yet to be well-documented.
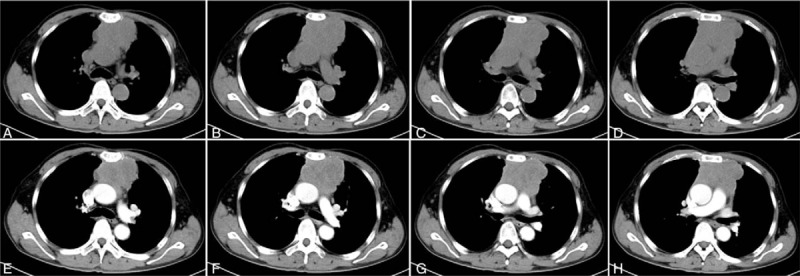
Patient concerns: A 57-year-old man presented with a 6-month history of continuous and progressive back pain. The patient, who had been diagnosed of thymic carcinoma (stage IV B) for 3 years, received surgical treatment of median sternotomy thymectomy, followed by 3 cycles of chemotherapy and 12 cycles of radiotherapy.
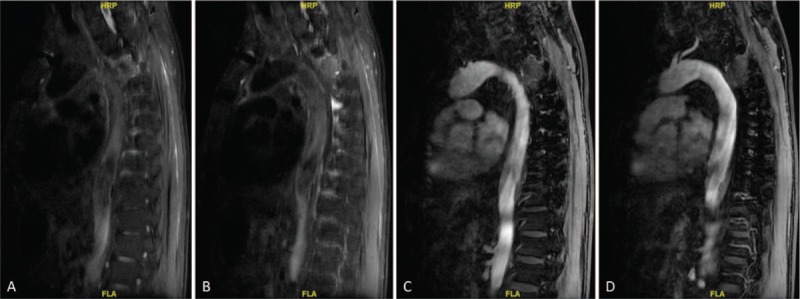
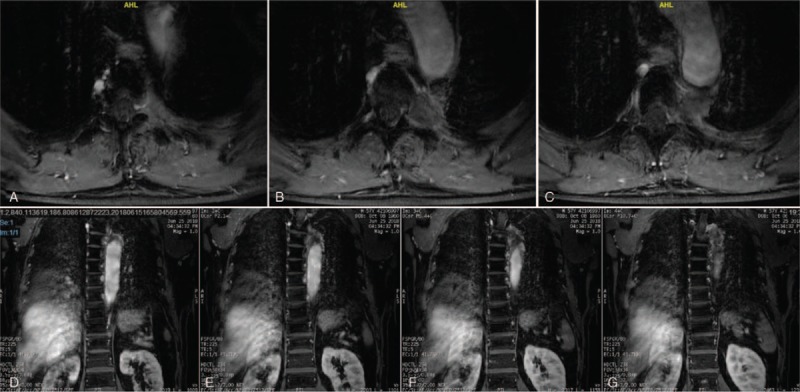
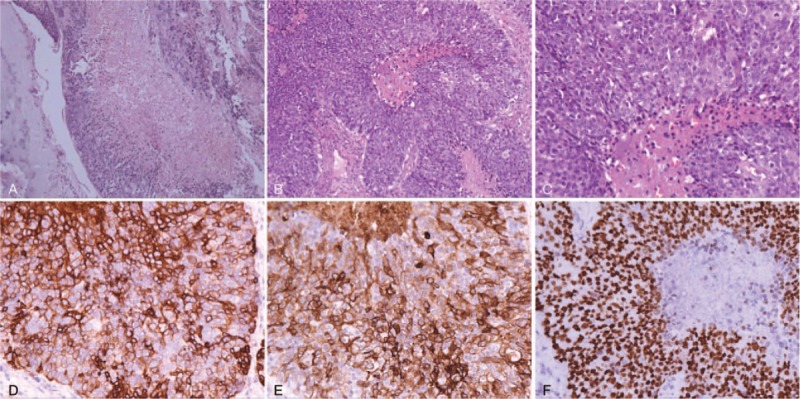
Diagnosis: Magnetic resonance imaging (MRI) of spine showed spinal cord compression secondary to the epidural component of the T4 mass, with increased metastatic marrow infiltration of the left T4 vetebral body, which presented as a solid tumor. Post-operative pathology confirmed the diagnosis of spinal metastases of thymic carcinoma.
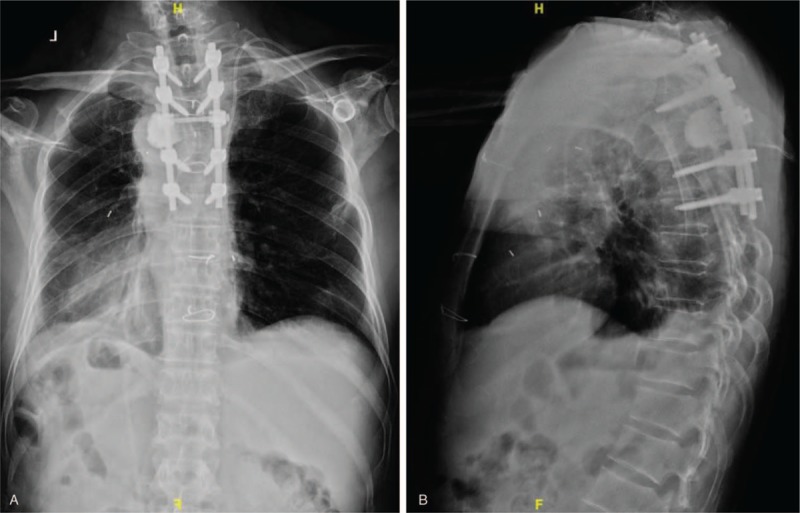
Interventions: The patient underwent exploratory surgery, circumferential spinal cord decompression, cement augmentation and a stabilization procedure via a posterior approach.
Outcomes: The patient's neurological deficits improved significantly after the surgery, and the postoperative period was uneventful at the 3-month follow-up visit. There were no other complications associated with the operation during the follow-up period.
Lessons: Taken together, the lesion's clinical features, imaging results, and pathological characteristics are unique. Combined efforts of specialists from orthopedics, neurosurgery, thoracic surgery, and medical oncology led to the successful diagnosis and management of this patient. Metastatic thymic carcinoma of the spine, although rare, should be part of the differential diagnosis when the patient has a history of thymic carcinoma and presents with back pain and radiculopathy. We recommend the posterior approach for spinal decompression of the metastatic thymic carcinoma when the tumor has caused neurological deficits. Osteoplasty by cement augmentation is also a good choice for surgical treatment.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
