

Laparoscopic pancreatoduodenectomy combined with portal-superior mesenteric vein resection and reconstruction with interposition graft: Case series
- PMID: 30653175
- PMCID: PMC6370126
- DOI: 10.1097/MD.0000000000014204
Laparoscopic pancreatoduodenectomy combined with portal-superior mesenteric vein resection and reconstruction with interposition graft: Case series
Abstract
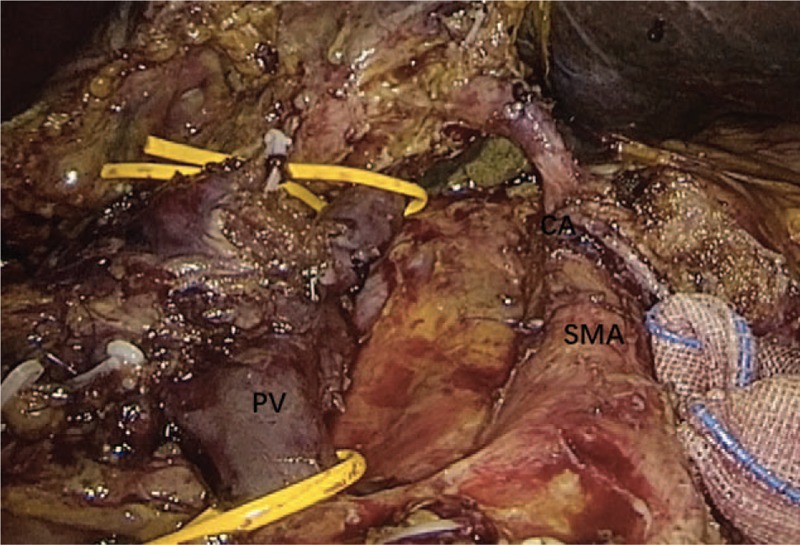
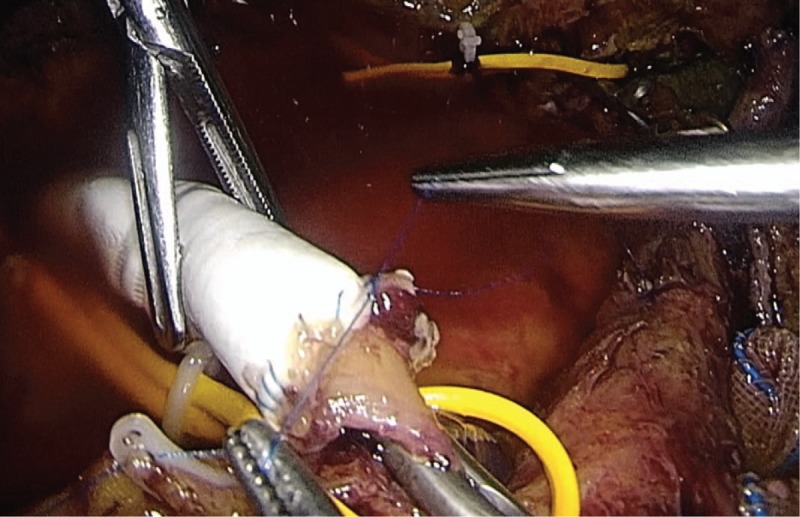
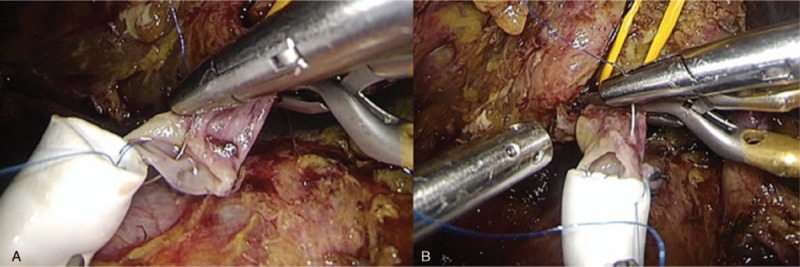
Rationale: With the development of laparoscopic techniques, laparoscopic pancreatoduodenectomy was applied in various indications including pancreatic cancer. Here, we share our experience of venous resection and reconstruction with interposition graft in laparoscopic pancreatoduodenectomy in these patients.
Patient concerns: We reviewed data of laparoscopic pancreatoduodenectomy with venous resection and reconstruction in patients with pancreatic cancer between the dates of October 2010 and November 2017.
Outcomes: Ten patients underwent laparoscopic pancreatoduodenectomy with portal-superior mesenteric vein resection and reconstruction with interposition graft. The mean operative time was 547 min. The mean blood loss was 435 ml. The mean length of venous defect after resection was 5.4 cm. R0 resection was achieved in nine patients (90%). There was one patient who suffered from severe postoperative complication. There was no 30-day mortality in this study. The long-term patency was achieved in all patients.
Conclusion: In this study, we demonstrate the initial experience of laparoscopic pancreaticoduodenectomy with long venous resection and reconstruction. Although applied in small number of patients, it could be another option for well-selected patients with reasonable morbidity and mortality as well as long-term outcomes in experienced minimally invasive surgical team.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Superior mesenteric-portal vein resection during laparoscopic pancreatoduodenectomy.Surg Endosc. 2017 Mar;31(3):1488-1495. doi: 10.1007/s00464-016-5115-3. Epub 2016 Jul 21. Surg Endosc. 2017. PMID: 27444832
-
Safety and efficacy of cryopreserved homologous veins for venous reconstruction in pancreatoduodenectomy.Surgery. 2017 Feb;161(2):385-393. doi: 10.1016/j.surg.2016.08.016. Epub 2016 Oct 7. Surgery. 2017. PMID: 27726914
-
Laparoscopic pancreaticoduodenectomy with major venous resection and reconstruction: anterior superior mesenteric artery first approach.Surg Endosc. 2018 Oct;32(10):4209-4215. doi: 10.1007/s00464-018-6167-3. Epub 2018 Mar 30. Surg Endosc. 2018. PMID: 29602996 Clinical Trial.
-
Laparoscopic pancreaticoduodenectomy with portal or superior mesenteric vein resection and reconstruction for pancreatic cancer: A single-center experience.Hepatobiliary Pancreat Dis Int. 2023 Apr;22(2):147-153. doi: 10.1016/j.hbpd.2023.01.004. Epub 2023 Jan 18. Hepatobiliary Pancreat Dis Int. 2023. PMID: 36690522 Review.
-
Left-sided portal hypertension after pancreatoduodenectomy with resection of the portal/superior mesenteric vein confluence. Results of a systematic review.Surgery. 2020 Sep;168(3):434-439. doi: 10.1016/j.surg.2020.04.030. Epub 2020 Jun 27. Surgery. 2020. PMID: 32600882
Cited by
-
The short- and long-term outcomes of laparoscopic pancreaticoduodenectomy combining with different type of mesentericoportal vein resection and reconstruction for pancreatic head adenocarcinoma: a Chinese multicenter retrospective cohort study.Surg Endosc. 2023 Jun;37(6):4381-4395. doi: 10.1007/s00464-023-09901-2. Epub 2023 Feb 9. Surg Endosc. 2023. PMID: 36759356
-
International expert consensus on laparoscopic pancreaticoduodenectomy.Hepatobiliary Surg Nutr. 2020 Aug;9(4):464-483. doi: 10.21037/hbsn-20-446. Hepatobiliary Surg Nutr. 2020. PMID: 32832497 Free PMC article. Review.
-
Laparoscopic Pancreaticoduodenectomy: Outcomes and Experience of 550 Patients in a Single Institution.Ann Surg Oncol. 2020 Oct;27(11):4562-4573. doi: 10.1245/s10434-020-08533-3. Epub 2020 May 7. Ann Surg Oncol. 2020. PMID: 32382892
-
Robotic Vascular Resection in Pancreatic Ductal Adenocarcinoma: A Systematic Review.J Clin Med. 2024 Mar 29;13(7):2000. doi: 10.3390/jcm13072000. J Clin Med. 2024. PMID: 38610766 Free PMC article. Review.
-
Tips and tricks for a safe laparoscopic pancreatoduodenectomy.Wideochir Inne Tech Maloinwazyjne. 2020 Sep;15(3):383-390. doi: 10.5114/wiitm.2020.97977. Epub 2020 Aug 17. Wideochir Inne Tech Maloinwazyjne. 2020. PMID: 32904617 Free PMC article. Review.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. - PubMed
-
- National Cancer Insitute. SEER Cancer Statistics Review, 1975–2009 (Vintage 2009 Populations). Available at: http://seer.cancer.gov/csr/1975_2009_pops09/.
-
- Barreto SG, Windsor JA. Justifying vein resection with pancreatoduodenectomy. Lancet Oncol 2016;17:e118–24. - PubMed
-
- Ohgi K, Yamamoto Y, Sugiura T, et al. Is pancreatic head cancer with portal venous involvement really borderline resectable? Appraisal of an upfront surgery series. Ann Surg Oncol 2017;24:2752–61. - PubMed
-
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology. Pancreatic Adenocarcinoma. Version 2.2017. http://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf Accessed May 20, 2017. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
