

Gastroschisis Trends and Ecologic Link to Opioid Prescription Rates - United States, 2006-2015
- PMID: 30653484
- PMCID: PMC6336188
- DOI: 10.15585/mmwr.mm6802a2
Gastroschisis Trends and Ecologic Link to Opioid Prescription Rates - United States, 2006-2015
Abstract
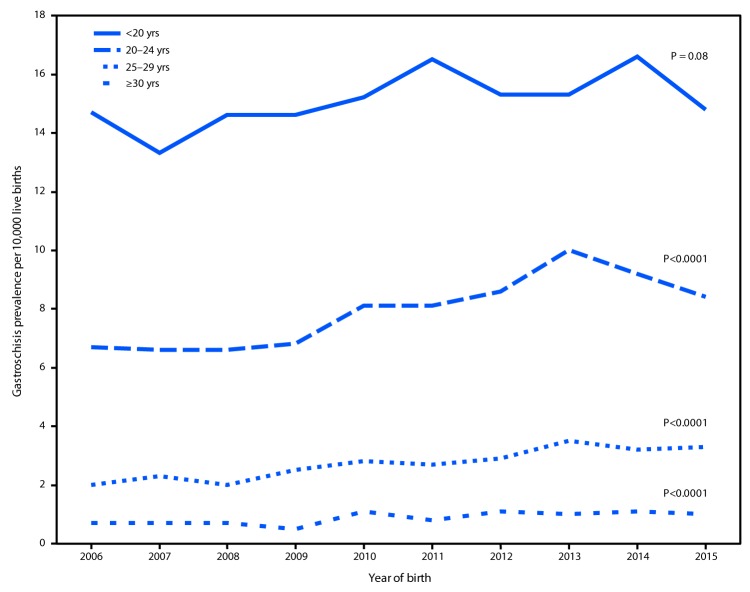
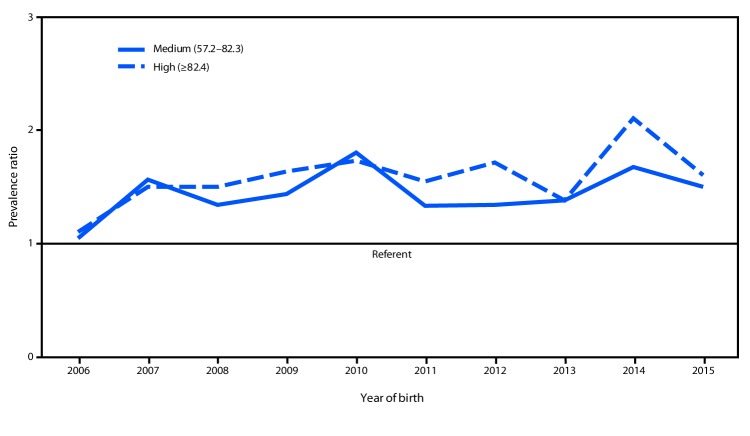
Prevalence of gastroschisis, a serious birth defect of the abdominal wall resulting in some of the abdominal contents extending outside the body at birth, has been increasing worldwide (1,2). Gastroschisis requires surgical repair after birth and is associated with digestive and feeding complications during infancy, which can affect development. Recent data from 14 U.S. states indicated an increasing prevalence of gastroschisis from 1995 to 2012 (1). Young maternal age has been strongly associated with gastroschisis, but research suggests that risk factors such as smoking, genitourinary infections, and prescription opioid use also might be associated (3-5). Data from 20 population-based state surveillance programs were pooled and analyzed to assess age-specific gastroschisis prevalence during two 5-year periods, 2006-2010 and 2011-2015, and an ecologic approach was used to compare annual gastroschisis prevalence by annual opioid prescription rate categories. Gastroschisis prevalence increased only slightly (10%) from 2006-2010 to 2011-2015 (prevalence ratio = 1.1, 95% confidence interval [CI] = 1.0-1.1), with the highest prevalence among mothers aged <20 years. During 2006-2015, the prevalence of gastroschisis was 1.6 times higher in counties with high opioid prescription rates (5.1 per 10,000 live births; CI = 4.9-5.3) and 1.4 times higher where opioid prescription rates were medium (4.6 per 10,000 live births; CI = 4.4-4.8) compared with areas with low prescription rates (3.2 per 10,000 live births; CI = 3.1-3.4). Public health research is needed to understand factors contributing to the association between young maternal age and gastroschisis and assess the effect of prescription opioid use during pregnancy on this pregnancy outcome.
Conflict of interest statement
All authors have completed and submitted the ICMJE form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Broussard CS, Rasmussen SA, Reefhuis J, et al. Maternal treatment with opioid analgesics and risk for birth defects. Am J Obstet Gynecol 2011;204:314 e1–11. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
