

Effect of structured self-monitoring of blood glucose, with and without additional TeleCare support, on overall glycaemic control in non-insulin treated Type 2 diabetes: the SMBG Study, a 12-month randomized controlled trial
- PMID: 30653704
- PMCID: PMC6593419
- DOI: 10.1111/dme.13899
Effect of structured self-monitoring of blood glucose, with and without additional TeleCare support, on overall glycaemic control in non-insulin treated Type 2 diabetes: the SMBG Study, a 12-month randomized controlled trial
Abstract
Aim: To examine the impact of structured self-monitoring of blood glucose, with or without TeleCare support, on glycaemic control in people with sub-optimally controlled Type 2 diabetes.
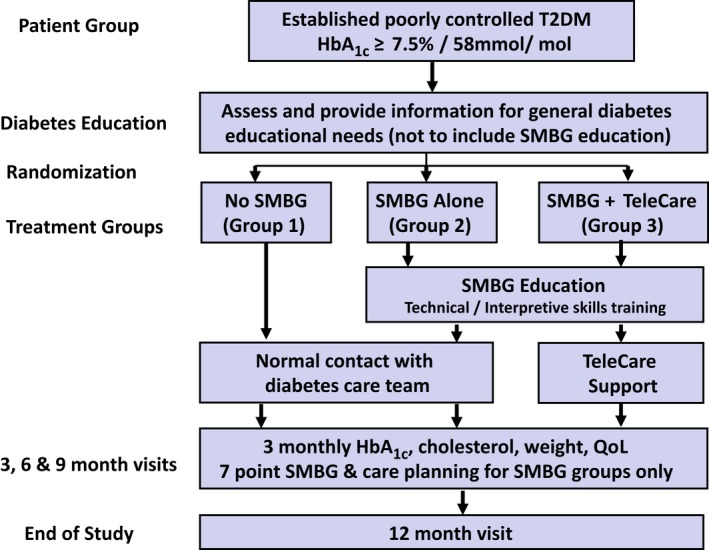
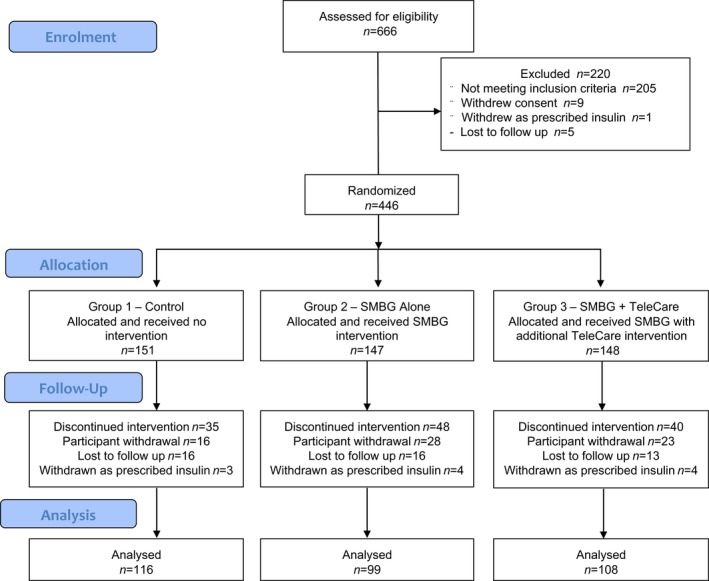
Methods: We conducted a 12-month, multicentre, randomized controlled trial in people with established (>1 year) Type 2 diabetes not on insulin therapy, with sub-optimal glycaemic control [HbA1c ≥58 to ≤119 mmol/mol (≥7.5% to ≤13%)]. A total of 446 participants were randomized to a control group (n =151) receiving usual diabetes care, a group using structured self-monitoring of blood glucose alone (n =147) or a group using structured self-monitoring of blood glucose with additional monthly 'TeleCare' support (n =148). The primary outcome was HbA1c at 12 months.
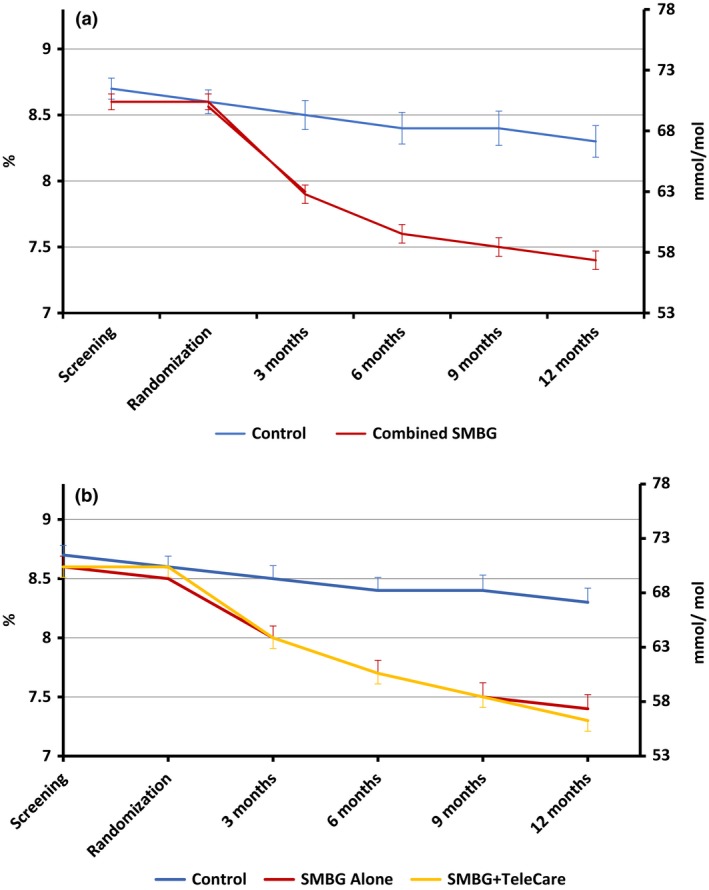
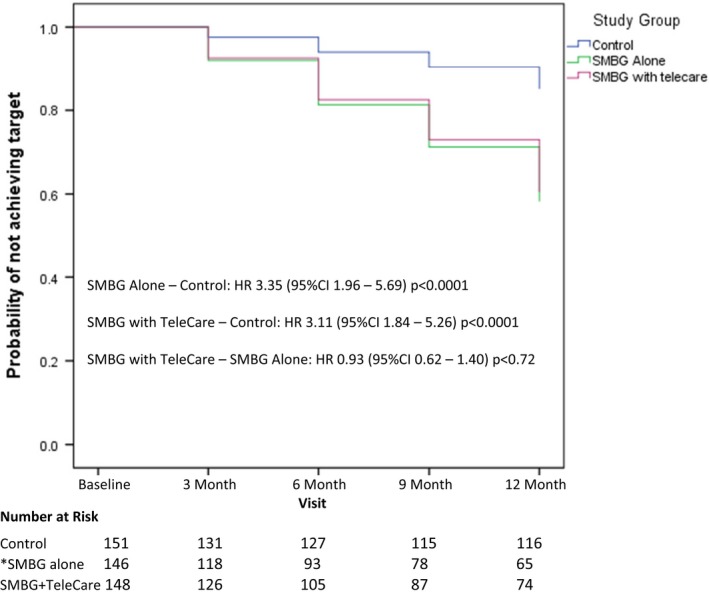
Results: A total of 323 participants (72%) completed the study; 116 (77%) in the control group, 99 (67%) in the self-monitoring of blood glucose alone group and 108 (73%) in the self-monitoring of blood glucose plus TeleCare group. Compared to baseline, the mean HbA1c was lower in all groups at 12 months, with reductions of 3.3 mmol/mol (95% CI -5.71 to -0.78) or 0.3% (95% CI -0.52 to -0.07; P=0.01) in the control group, 11.4 mmol/mol (95% CI -14.11 to -8.76) or 1.1% (-1.29 to -0.81; P<0.0001) in the group using self-monitoring of blood glucose alone and 12.8 mmol/mol (95% CI -15.34 to -10.31) or 1.2% (95% CI -1.40 to -0.94; P<0.0001) in the group using self-monitoring of blood glucose plus TeleCare. This represents a reduction in HbA1c of 8.9 mmol/mol (95% CI -11.97 to -5.84) or 0.8% (95% CI -1.10 to -0.54; P≤0.0001) with structured self-monitoring of blood glucose compared to the control group. Participants with lower baseline HbA1c , shorter duration of diabetes and higher educational achievement were more likely to achieve HbA1c ≤53 mmol/mol (7.0%).
Conclusions: Structured self-monitoring of blood glucose provides clinical and statistical improvements in glycaemic control in Type 2 diabetes. No additional benefit, over and above the use of structured self-monitoring of blood glucose, was observed in glycaemic control with the addition of once-monthly TeleCare support. (Clinical trial registration no.: ISRCTN21390608).
© 2019 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK.
Figures
References
-
- Machry RV, Rados DV, Gregorio GR, Rodrigues TC. Self‐monitoring blood glucose improves glycaemic control in type 2 diabetes without intensive treatment: a systematic review and meta‐analysis. Diabetes Res Clin Pract 2018; 142: 173–187. - PubMed
-
- Cohen M, Zimmet P. Self‐monitoring of blood glucose levels in non‐insulin‐dependent diabetes mellitus. Med. J. Aust 1983; 2: 377–380. - PubMed
-
- Davidson MB, Castellanos M, Kain D, Duran P. The effect of self‐monitoring of blood glucose concentrations on glycated hemoglobin levels in diabetic patients not taking insulin: a blinded, randomized trial. Am J Med 2005; 118: 422–425. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
