

Liraglutide effects in a paediatric (7-11 y) population with obesity: A randomized, double-blind, placebo-controlled, short-term trial to assess safety, tolerability, pharmacokinetics, and pharmacodynamics
- PMID: 30653847
- PMCID: PMC6590663
- DOI: 10.1111/ijpo.12495
Liraglutide effects in a paediatric (7-11 y) population with obesity: A randomized, double-blind, placebo-controlled, short-term trial to assess safety, tolerability, pharmacokinetics, and pharmacodynamics
Abstract
Background: Childhood obesity is a major public health concern with limited treatment options.
Objective: The aim of this study was to assess safety, tolerability, pharmacokinetics, and pharmacodynamics during short-term treatment with liraglutide in children (7-11 y) with obesity.
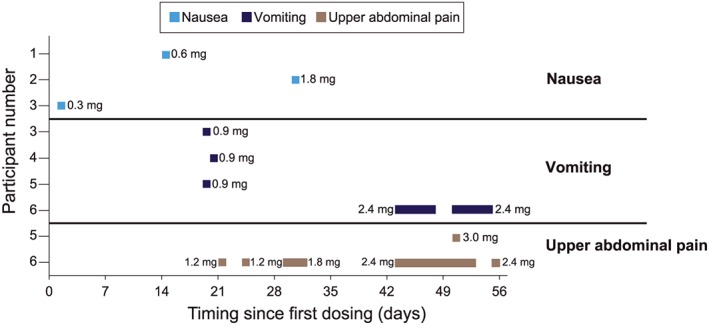
Methods: In this randomized, double-blind, placebo-controlled trial, 24 children received at least one dose of once-daily subcutaneous liraglutide (n = 16) or placebo (n = 8) starting at 0.3 mg with weekly dose escalations up to 3.0 mg or maximum tolerated dose, and 20 children completed the trial (14 in the liraglutide group and six in the placebo group). The primary endpoint was the number of adverse events.
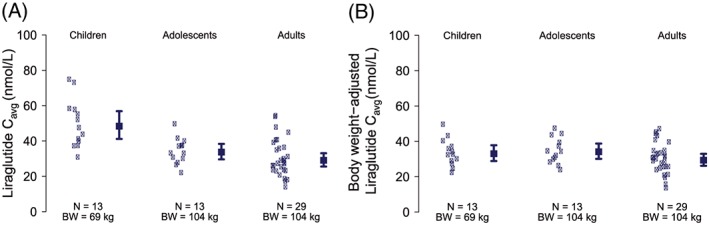
Results: Baseline characteristics (mean ± standard deviation) included the following: age 9.9 ± 1.1 years, weight 71.5 ± 15.4 kg, and 62.5% male. Thirty-seven adverse events were reported in nine liraglutide-treated participants (56.3%) versus 12 events in five placebo-treated participants (62.5%). Most adverse events were mild in severity, three were of moderate severity, and none were severe. Gastrointestinal disorders were the most frequently reported events occurring in 37.5% of liraglutide-treated participants compared with placebo (12.5%). Six asymptomatic hypoglycaemic episodes occurred in five participants of whom four were liraglutide treated. Liraglutide exposure was consistent with dose proportionality. Body weight was the only covariate to significantly impact exposure. A significant reduction in body mass index (BMI) Z score from baseline to end of treatment (estimated treatment difference: -0.28; P = 0.0062) was observed.
Conclusion: Short-term treatment with liraglutide in children with obesity revealed a safety and tolerability profile similar to trials in adults and adolescents with obesity, with no new safety issues.
Keywords: Clinical trial; GLP-1; liraglutide; paediatric.
© 2019 The Authors. Pediatric Obesity published by John Wiley & Sons Ltd on behalf of World Obesity Federation.
Conflict of interest statement
This study was sponsored by Novo Nordisk, which was responsible for the overall trial design, conduct, and analysis and provided a formal review of the manuscript, but the authors had final authority, including choice of journal and the decision to submit the work for publication. L.D.M. serves as site principal investigator for clinical trials supported by Novo Nordisk, AstraZeneca, and Sanofi Aventis. She serves on the oversight committee for the Pediatric Diabetes Consortium. L.W., K.C.C.P., P.M.H., and H.K.H. are employees of Novo Nordisk. K.C.C.P., P.M.H., and H.K.H. own stocks in Novo Nordisk. R.A.R. has no disclosures to report.
Figures
References
-
- Ogden CL, Carroll M. Prevalence of obesity among children and adolescents: United States, trends 1963‐1965 through 2007‐2008. Health E‐Stat. June 2010. Available from: https://www.cdc.gov/nchs/data/hestat/obesity_child_07_08/obesity_child_0....
-
- Kumar S, Kelly AS. Review of childhood obesity: from epidemiology, etiology, and comorbidities to clinical assessment and treatment. Mayo Clinic Proc. 2017;92:251–265. - PubMed
-
- Wabitsch M. Overweight and obesity in European children: definition and diagnostic procedures, risk factors and consequences for later health outcome. Eur J Pediatr. 2000;159:S8–S13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
