

Long-Term Impact of Iatrogenic Bile Duct Injury
- PMID: 30654363
- PMCID: PMC7026941
- DOI: 10.1159/000496432
Long-Term Impact of Iatrogenic Bile Duct Injury
Abstract
Background: Bile duct injury (BDI) is a devastating complication following cholecystectomy. After initial management of BDI, patients stay at risk for late complications including anastomotic strictures, recurrent cholangitis, and secondary biliary cirrhosis.
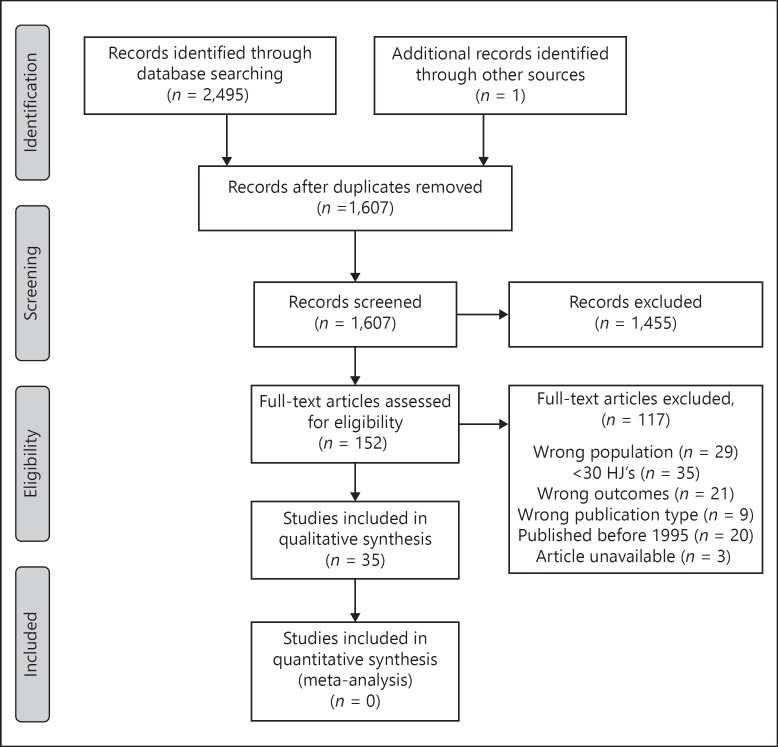
Methods: We provide a comprehensive overview of current literature on the long-term outcome of BDI. Considering the availability of only limited data regarding treatment of anastomotic strictures in literature, we also retrospectively analyzed patients with anastomotic strictures following a hepaticojejunostomy (HJ) from a prospectively maintained database of 836 BDI patients.
Results: Although clinical outcomes of endoscopic, radiologic, and surgical treatment of BDI are good with success rates of around 90%, quality of life (QoL) may be impaired even after "clinically successful" treatment. Following surgical treatment, the incidence of anastomotic strictures varies from 5 to 69%, with most studies reporting incidences around 10-20%. The median time to stricture formation varies between 11 and 30 months. Long-term BDI-related mortality varies between 1.8 and 4.6%. Of 91 patients treated in our center for anastomotic strictures after HJ, 81 (89%) were treated by percutaneous balloon dilatation, with a long-term success rate of 77%. Twenty-four patients primarily or secondarily underwent surgical revision, with recurrent strictures occurring in 21%.
Conclusions: The long-term impact of BDI is considerable, both in terms of clinical outcomes and QoL. Treatment should be performed in tertiary expert centers to optimize outcomes. Patients require a long-term follow-up to detect anastomotic strictures. Strictures should initially be managed by percutaneous dilatation, with surgical revision as a next step in treatment.
Keywords: Anastomotic stricture; Bile duct injury; Bile leakage; Cholecystectomy; Long-term outcome.
© 2019 The Author(s) Published by S. Karger AG, Basel.
Conflict of interest statement
The authors declare that they have no conflicts of interest to disclose.
Figures
References
-
- Calvete J, Sabater L, Camps B, Verdu A, Gomez-Portilla A, Martin J, et al. Bile duct injury during laparoscopic cholecystectomy: myth or reality of the learning curve? Surg Endosc. 2000;14:608–611. - PubMed
-
- Halbert C, Pagkratis S, Yang J, Meng Z, Altieri MS, Parikh P, et al. Beyond the learning curve incidence of bile duct injuries following laparoscopic cholecystectomy normalize to open in the modern era. Surg Endosc. 2016;30:2239–2243. - PubMed
-
- Mangieri CW, Hendren BP, Strode MA, Bandera BC, Faler BJ. Bile duct injuries (BDI) in the advanced laparoscopic cholecystectomy era. Surg Endosc. 2018 Epub ahead of print. - PubMed
-
- Rystedt J, Lindell G, Montgomery A. Bile duct injuries associated with 55,134 cholecystectomies: treatment and outcome from a National perspective. World J Surg. 2016;40:73–80. - PubMed
