

The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data
- PMID: 30654773
- PMCID: PMC6337770
- DOI: 10.1186/s12906-018-2409-0
The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data
Abstract
Background: Peppermint oil (PO) has intrinsic properties that may benefit patients with irritable bowel syndrome (IBS) symptoms. The study objective was to determine the effect of peppermint oil in the treatment of the IBS.
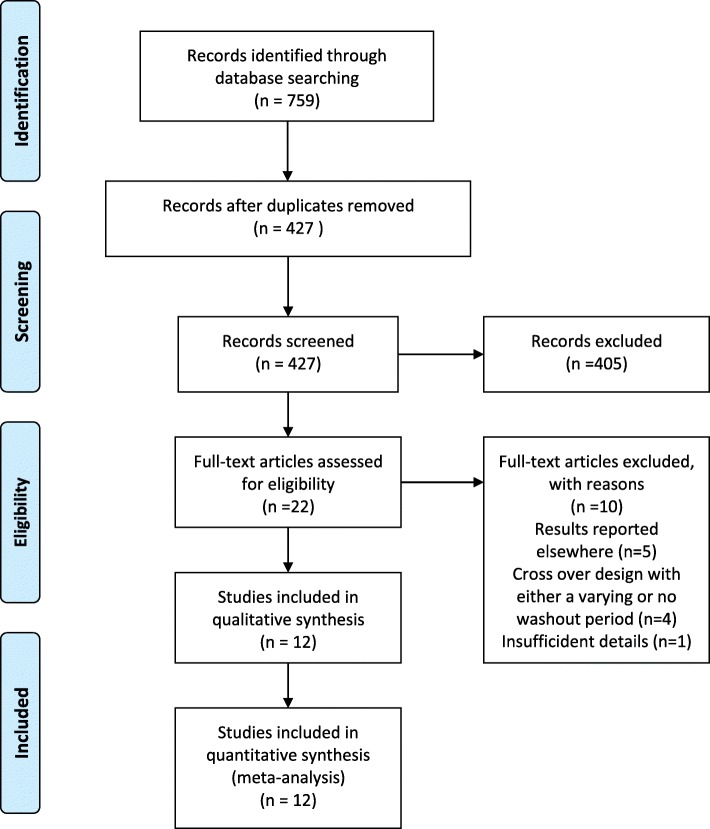
Methods: We systematically searched MEDLINE (PubMed), Cochrane Central Register of Controlled Trials (Cochrane CENTRAL), ClinicalTrials.gov, EMBASE (Ovid), and Web of Science for randomized controlled trials (RCTs) of PO for IBS. We appraised the eligible studies by the Cochrane risk of bias tool. We performed random-effects meta-analysis on primary outcomes including global improvement in IBS symptoms and abdominal pain. A PRISMA-compliant study protocol is registered in PROSPERO Register [2016, CRD42016050917].
Results: Twelve randomized trials with 835 patients were included. For global symptom improvement, the risk ratio (RR) from seven RCTs for the effect of PO (n = 253) versus placebo (n = 254) on global symptoms was 2.39 [95% confidence interval (CI): 1.93, 2.97], I2 = 0%, z = 7.93 (p < 0.00001). Regarding abdominal pain, the RR from six RCTs for the effect of PO (n = 278) versus placebo (n = 278) was 1.78 [95% CI: 1.43, 2.20], I2 = 0%, z = 5.23 (p < 0.00001). Overall, there were no differences in the reported adverse effects: PO (32 events, 344 total, 9.3%) versus placebo (20 events, 327 total, 6.1%) for eight RCTs; RR 1.40 [95% CI: 0.87, 2.26] I2 = 0%, z = 1.39 (p = 0.16). The number needed to treat with PO to prevent one patient from having persistent symptoms was three for global symptoms and four for abdominal pain.
Conclusions: In the most comprehensive meta-analysis to date, PO was shown to be a safe and effective therapy for pain and global symptoms in adults with IBS.
Keywords: Abdominal pain; Global symptom relief; IBS; Irritable bowel syndrome; Meta-analysis; PRISMA; Peppermint oil.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Dr. Mullin is an Associate Editor of BMC Complementary and Alternative Medicine.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
 ,
, ,
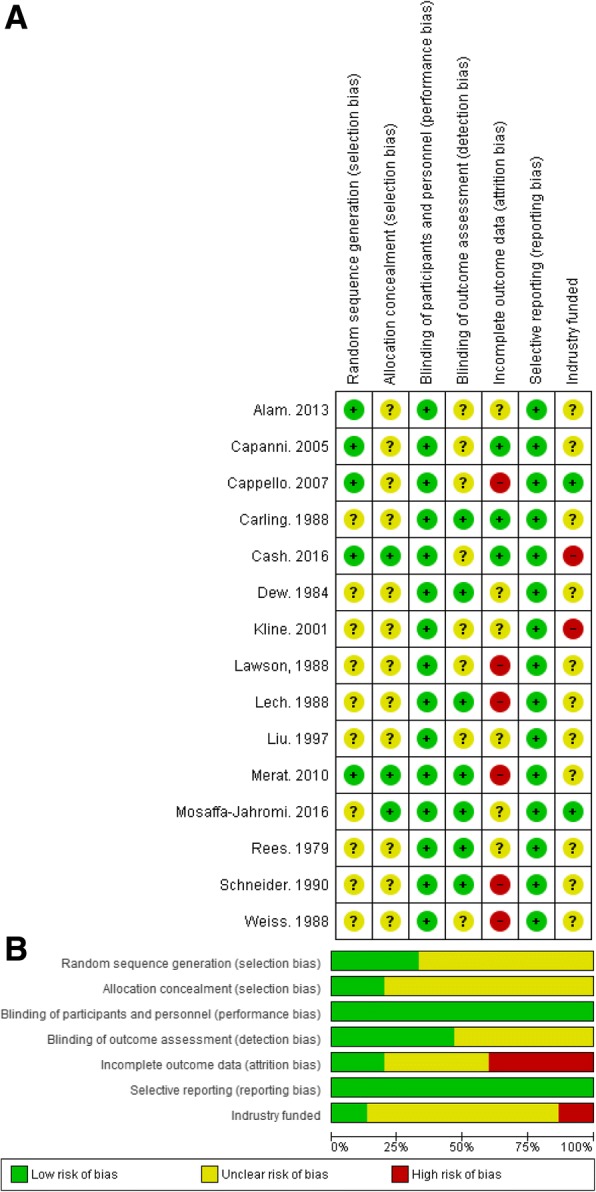
, denote low, unclear, and high risk of bias, respectively. Six of the 12 studies were assessed as having high risk of attrition bias and two studies were funded by industry (high risk of bias). Ten of the 12 included studies did not report random sequence generation and allocation concealment (unclear risk of selection bias). In contrast, the blinding of participants and personnel were well performed (low risk of performance bias in seven of the 12 included studies). Selective reporting was not observed in any studies (low risk if bias). Figure 2b shows the overall risk of bias by domain: the risk of bias is displayed as low risk (green, +), unclear (yellow,?), or high risk (red, −)
denote low, unclear, and high risk of bias, respectively. Six of the 12 studies were assessed as having high risk of attrition bias and two studies were funded by industry (high risk of bias). Ten of the 12 included studies did not report random sequence generation and allocation concealment (unclear risk of selection bias). In contrast, the blinding of participants and personnel were well performed (low risk of performance bias in seven of the 12 included studies). Selective reporting was not observed in any studies (low risk if bias). Figure 2b shows the overall risk of bias by domain: the risk of bias is displayed as low risk (green, +), unclear (yellow,?), or high risk (red, −)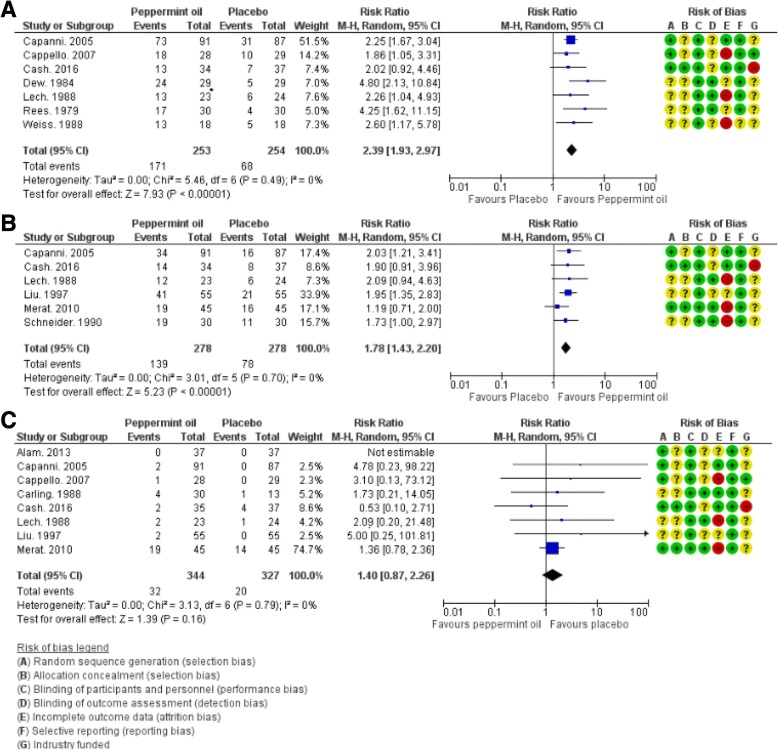
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
