

Patterns and risk of recurrence in patients with esophageal cancer with a pathologic complete response after chemoradiotherapy followed by surgery
- PMID: 30655068
- PMCID: PMC6534488
- DOI: 10.1016/j.jtcvs.2018.09.136
Patterns and risk of recurrence in patients with esophageal cancer with a pathologic complete response after chemoradiotherapy followed by surgery
Abstract
Objectives: A pathologic complete response in patients with locally advanced esophageal cancer after chemoradiotherapy and surgery is associated with improved overall and disease-free survival. Nevertheless, approximately one third of patients with a pathologic complete response still have a recurrence. The aim of this study was to evaluate risk factors and patterns of recurrence in patients with locally advanced esophageal cancer who achieved a pathologic complete response after chemoradiotherapy and surgery.
Methods: We performed a retrospective review of a single-institution database of 233 patients with stage II and III esophageal cancer with a pathologic complete response after chemoradiotherapy and surgery between 1997 and 2017. A multivariable competing risk-regression model was used to identify predictors of recurrence.
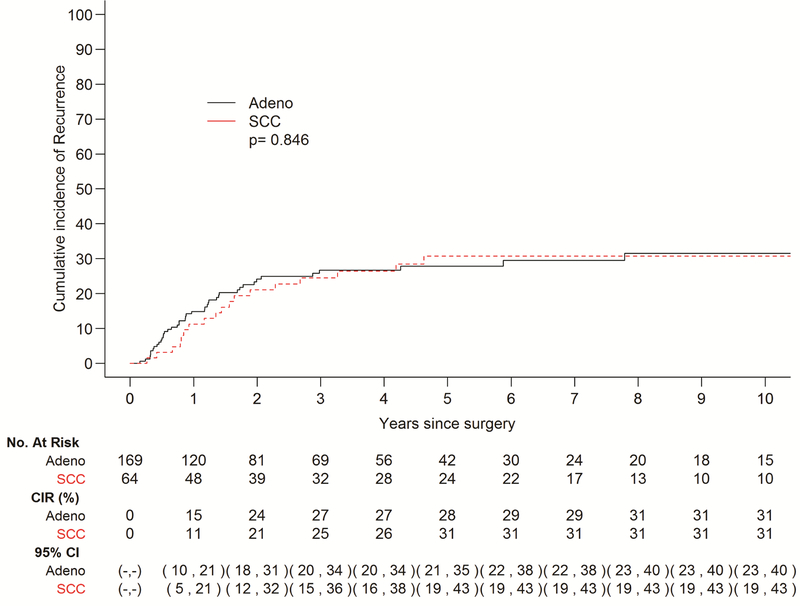
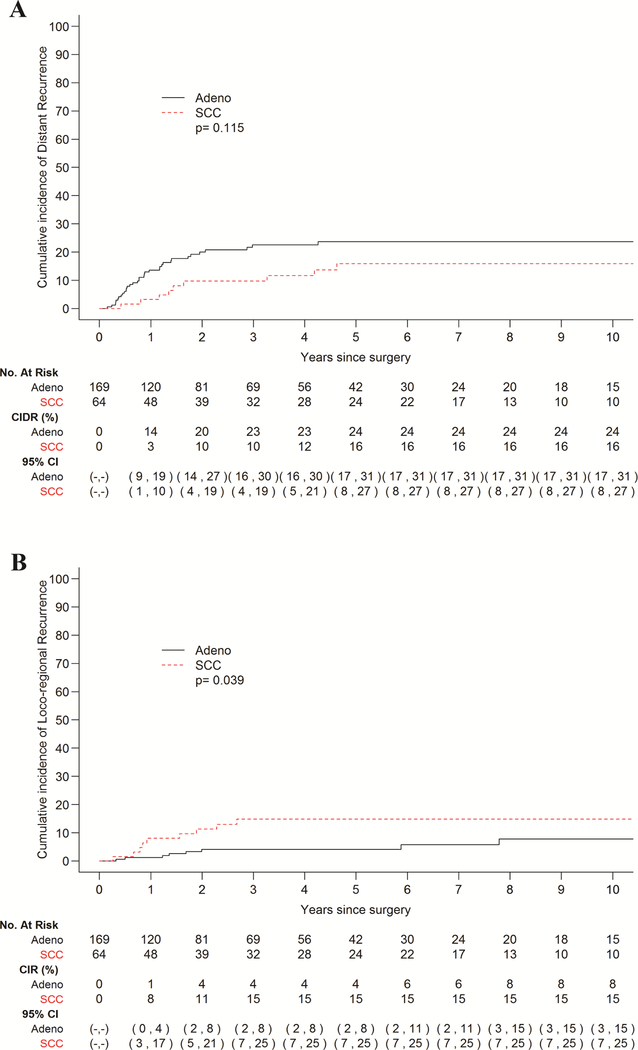
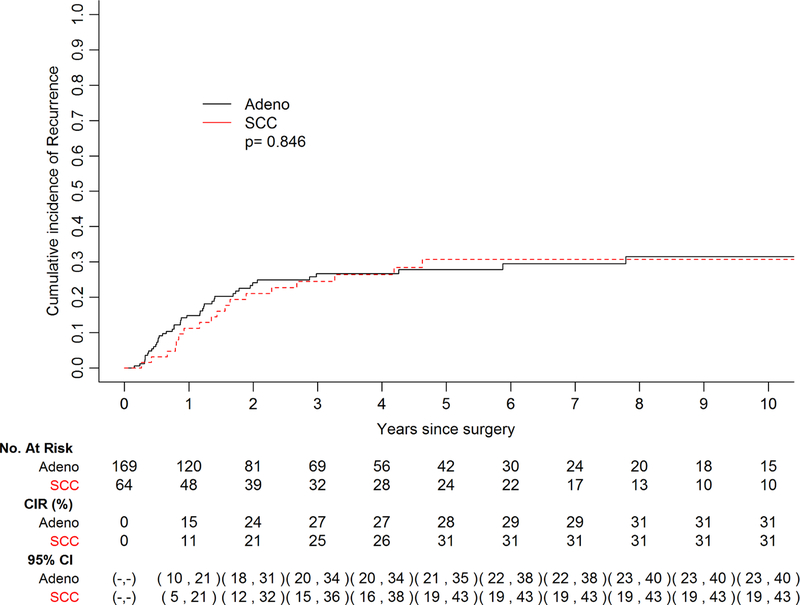
Results: A total of 61 patients exhibited recurrence in this cohort, 43 with adenocarcinoma and 18 with squamous cell carcinoma. Five-year cumulative incidence of recurrence did not vary by histology. Univariable analysis revealed that poor tumor differentiation (hazard ratio, 2.28; P = .022) and advanced clinical stage (hazard ratio, 1.89; P = .042) are predictors of recurrence in the esophageal adenocarcinoma subgroup, whereas poor tumor differentiation remained the only independent predictor on multivariable analysis in the entire cohort (hazard ratio, 2.28; P = .009). Patients with esophageal adenocarcinoma had a higher incidence of distant recurrences, and patients with esophageal squamous cell carcinoma demonstrated a higher incidence of loco-regional recurrence (P = .039).
Conclusions: Poor tumor differentiation is an independent risk factor for recurrence in patients with esophageal cancer with a pathologic complete response. Although there is no difference in the cumulative incidence of recurrence between esophageal adenocarcinoma and esophageal squamous cell carcinoma, patterns of recurrence appear to differ. Thus, treatment and surveillance strategies may be tailored appropriately.
Keywords: esophageal cancer; neoadjuvant chemoradiotherapy plus surgery; pathologic complete response; recurrence; survival.
Copyright © 2018 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Recurrence in complete responders after trimodality therapy in esophageal cancer.J Thorac Dis. 2019 May;11(Suppl 9):S1304-S1306. doi: 10.21037/jtd.2019.04.77. J Thorac Dis. 2019. PMID: 31245116 Free PMC article. No abstract available.
References
-
- van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012;366:2074–2084. - PubMed
-
- Gebski V, Burmeister B, Smithers BM, Foo K, Zalcberg J, Simes J. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: a meta-analysis. The Lancet Oncology 2007;8:226–234. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
