

Transient Ischemic Attack and Carotid Web
- PMID: 30655258
- PMCID: PMC7028627
- DOI: 10.3174/ajnr.A5946
Transient Ischemic Attack and Carotid Web
Abstract
Background and purpose: Carotid web was recognized as a cause of ischemic stroke. We sought to determine the clinical and imaging profiles of patients with a carotid web as well as its association with TIA.
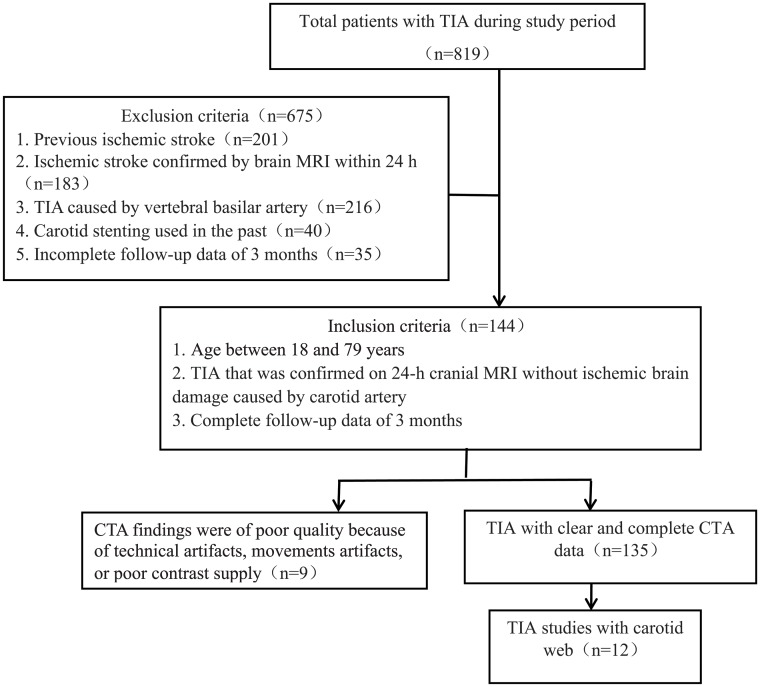
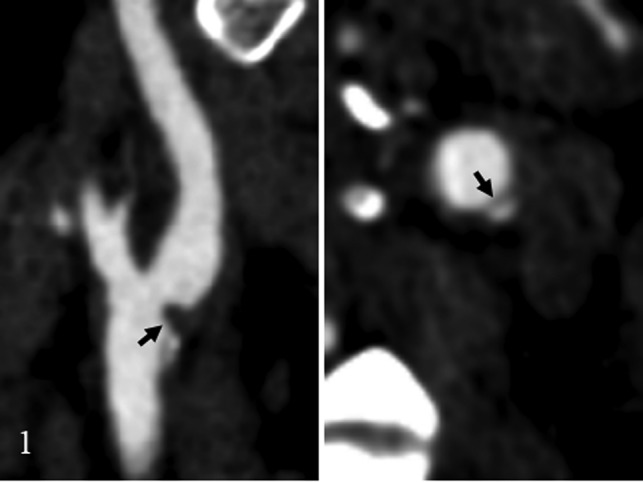
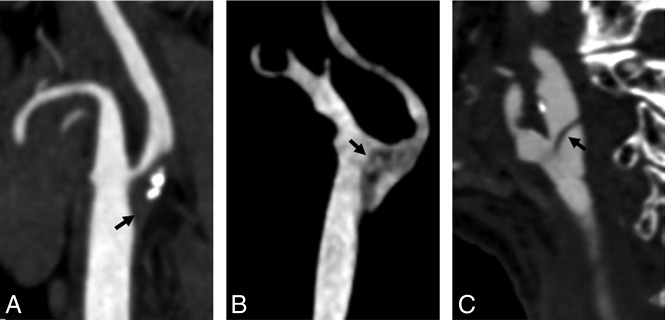
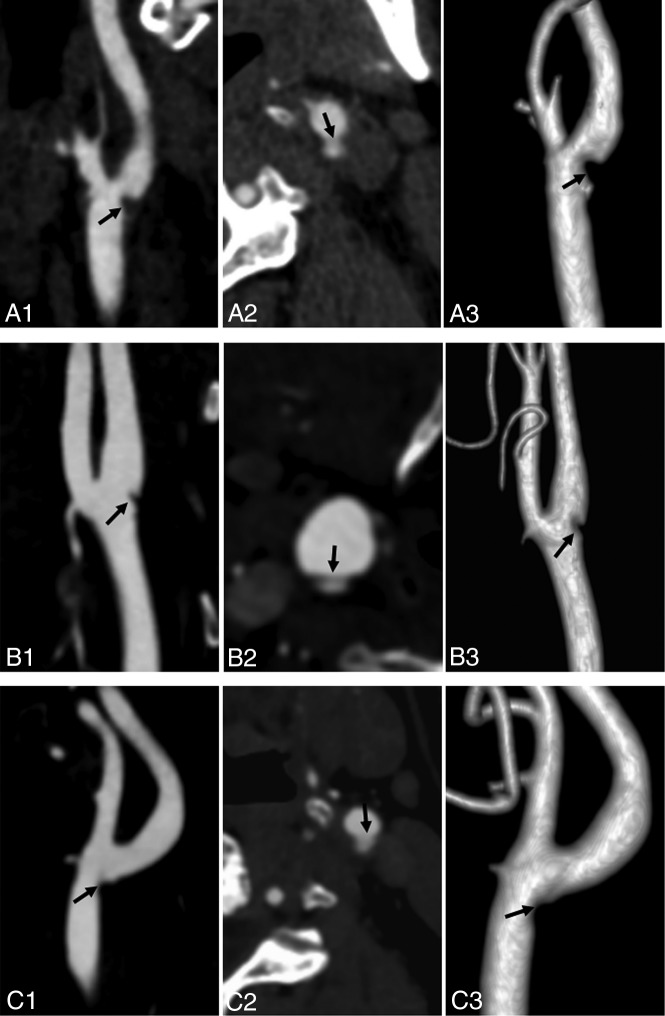
Materials and methods: A retrospective review of carotid CT angiography studies and brain MR imaging in patients with TIA during the past 3 years (n = 135) was performed to determine the presence of carotid webs by 2 experienced neuroradiologists according to previously published criteria. Demographics and clinical and imaging characteristics are shown by descriptive statistics for patients with an identified carotid web. The agreement in the detection of carotid webs between 2 neuroradiologists was examined using κ statistics.
Results: There were 12 (8.9%) carotid webs at the symptomatic bifurcation and 1 carotid web (0.7%) at the asymptomatic bifurcation, and no hyperintensity was seen on DWI of these 12 patients. Eight of these 12 (75%) patients with a carotid web were women. None of the 12 patients with a carotid web had major risk factors or other causes of TIA. Fair-to-good interobserver agreement (κ = 0.87) was seen for diagnosing a carotid web with CT angiography. The rate (10/12, 83.3%) of short-term recurrent episodes of TIA in patients with TIA with a carotid web was significantly higher than that of patients without a carotid web (15/123, 12.2%) (P < .001).
Conclusions: The incidence of carotid web in patients with TIA was 8.9%. There is an association between carotid web and patients with TIA without other identified risks. Carotid web may be an underestimated risk factor for TIA.
© 2019 by American Journal of Neuroradiology.
Figures
References
-
- Easton JD, Saver JL, Albers GW, et al. ; American Heart Association, American Stroke Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Interdisciplinary Council on Peripheral Vascular Disease. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease—The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009;40:2276–93 10.1161/STROKEAHA.108.192218 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous