

The ADAMTS13-VWF axis is dysregulated in chronic thromboembolic pulmonary hypertension
- PMID: 30655285
- PMCID: PMC6437602
- DOI: 10.1183/13993003.01805-2018
The ADAMTS13-VWF axis is dysregulated in chronic thromboembolic pulmonary hypertension
Abstract
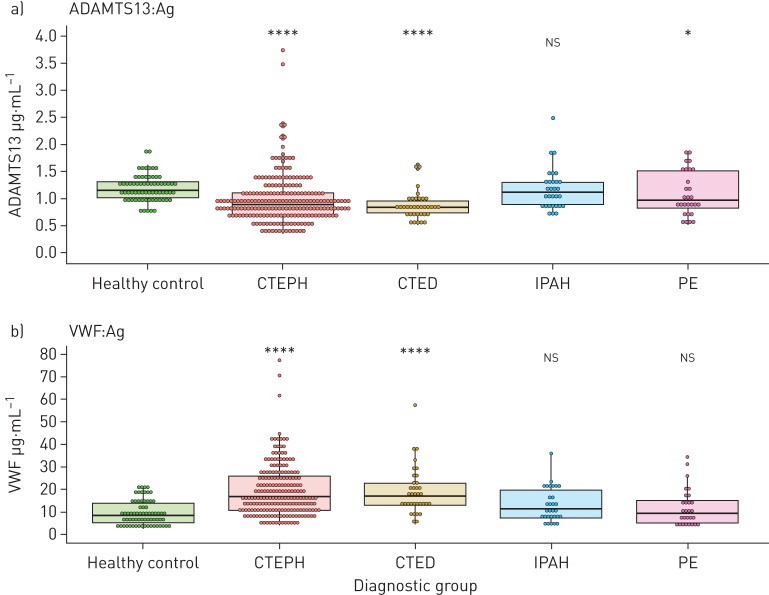
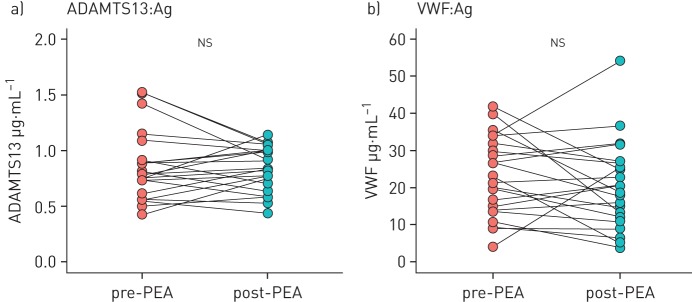
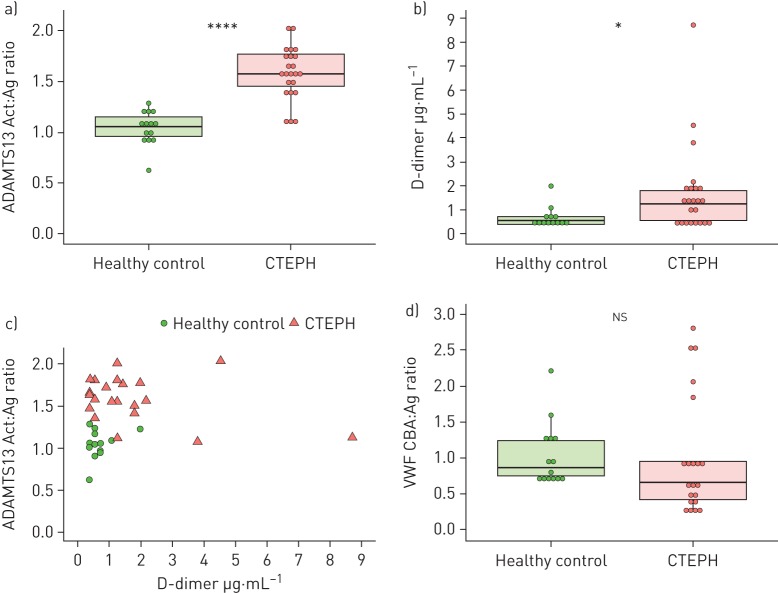
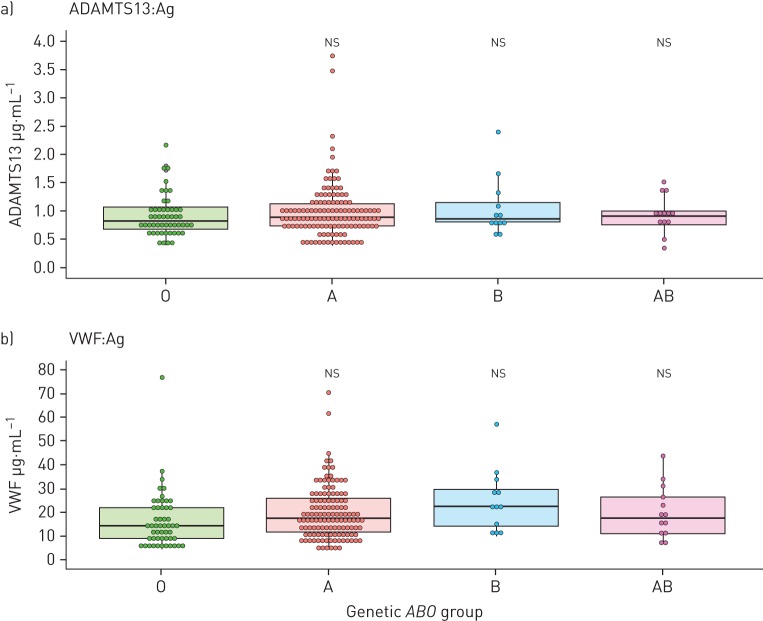
Chronic thromboembolic pulmonary hypertension (CTEPH) is an important consequence of pulmonary embolism that is associated with abnormalities in haemostasis. We investigated the ADAMTS13-von Willebrand factor (VWF) axis in CTEPH, including its relationship with disease severity, inflammation, ABO groups and ADAMTS13 genetic variants.ADAMTS13 and VWF plasma antigen levels were measured in patients with CTEPH (n=208), chronic thromboembolic disease without pulmonary hypertension (CTED) (n=35), resolved pulmonary embolism (n=28), idiopathic pulmonary arterial hypertension (n=30) and healthy controls (n=68). CTEPH genetic ABO associations and protein quantitative trait loci were investigated. ADAMTS13-VWF axis abnormalities were assessed in CTEPH and healthy control subsets by measuring ADAMTS13 activity, D-dimers and VWF multimeric size.Patients with CTEPH had decreased ADAMTS13 (adjusted β -23.4%, 95% CI -30.9- -15.1%, p<0.001) and increased VWF levels (β +75.5%, 95% CI 44.8-113%, p<0.001) compared to healthy controls. ADAMTS13 levels remained low after reversal of pulmonary hypertension by pulmonary endarterectomy surgery and were equally reduced in CTED. We identified a genetic variant near the ADAMTS13 gene associated with ADAMTS13 protein that accounted for ∼8% of the variation in levels.The ADAMTS13-VWF axis is dysregulated in CTEPH. This is unrelated to pulmonary hypertension, disease severity or markers of systemic inflammation and implicates the ADAMTS13-VWF axis in CTEPH pathobiology.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: M. Newnham reports education support (travel, registration and accommodation) to attend conferences from MSD and GSK, outside the submitted work. Conflict of interest: K. South has nothing to disclose. Conflict of interest: M. Bleda has nothing to disclose. Conflict of interest: W.R. Auger reports grants and non-financial support for advisory board work (travel support only) from Bayer, outside the submitted work. Conflict of interest: J.A. Barberà has nothing to disclose. Conflict of interest: H. Bogaard has nothing to disclose. Conflict of interest: K. Bunclark has nothing to disclose. Conflict of interest: J.E. Cannon reports grants for educational meetings from Actelion, GSK and MSD, outside the submitted work. Conflict of interest: M. Delcroix has nothing to disclose. Conflict of interest: C. Hadinnapola has nothing to disclose. Conflict of interest: L.S. Howard reports grants from Bayer PLC, during the conduct of the study. Conflict of interest: D. Jenkins reports grants and personal fees from Bayer, and personal fees from Actelion, outside the submitted work. Conflict of interest: E. Mayer reports speaker and consultancy fees from Actelion, Bayer and MSD, and speaker fees from Pfizer, outside the submitted work. Conflict of interest: C. Ng has nothing to disclose. Conflict of interest: C.J. Rhodes has nothing to disclose. Conflict of interest: N. Screaton has nothing to disclose. Conflict of interest: K. Sheares reports educational support (travel, registration and accommodation) to attend conferences from Actelion, Bayer, MSD and GSK, and has been on an advisory board for Actelion, outside the submitted work. Conflict of interest: M.A. Simpson has a contract of service with Genomics PLC, outside the submitted work. Conflict of interest: M. Southwood has nothing to disclose. Conflict of interest: L. Su has nothing to disclose. Conflict of interest: D. Taboada reports speaker honoraria and education/travel grants from Actelion, Bayer, GlaxoSmithKline, Lilly, MDS and Pfizer, outside the submitted work. Conflict of interest: M. Traylor has nothing to disclose. Conflict of interest: R.C. Trembath has nothing to disclose. Conflict of interest: S.S. Villar has nothing to disclose. Conflict of interest: M.R. Wilkins has nothing to disclose. Conflict of interest: J. Wharton reports personal fees for advisory board work from Actelion Pharmaceuticals Ltd, outside the submitted work. Conflict of interest: S. Gräf has nothing to disclose. Conflict of interest: J. Pepke-Zaba (or her institution) has received research/educational grants and has been serving on advisory boards for Actelion, Bayer, Merck and GSK. Conflict of interest: M. Laffan reports grants from British Heart Foundation during the conduct of the study; and support to attend conferences from Shire, outside the submitted work. Conflict of interest: D.A. Lane has nothing to disclose. Conflict of interest: N.W. Morrell has nothing to disclose. Conflict of interest: M. Toshner reports grants and personal fees from Bayer, Merck and Actelion, personal fees from GSK, and grants from Roche, during the conduct of the study.
Figures
References
-
- Ende-Verhaar YM, Cannegieter SC, Vonk Noordegraaf A, et al. . Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a contemporary view of the published literature. Eur Respir J 2017; 49: 1601792. - PubMed
-
- Moser KM, Bloor CM. Pulmonary vascular lesions occurring in patients with chronic major vessel thromboembolic pulmonary hypertension. Chest 1993; 103: 685–692. - PubMed
-
- Galiè N, Kim HS. Pulmonary microvascular disease in chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc 2006; 3: 571. - PubMed
-
- Satoh T, Satoh K, Yaoita N, et al. . Activated TAFI promotes the development of chronic thromboembolic pulmonary hypertension: a possible novel therapeutic target. Circ Res 2017; 120: 1246–1262. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous