

Whole-Exome Sequencing Enables a Precision Medicine Approach for Kidney Transplant Recipients
- PMID: 30655312
- PMCID: PMC6362619
- DOI: 10.1681/ASN.2018060575
Whole-Exome Sequencing Enables a Precision Medicine Approach for Kidney Transplant Recipients
Abstract
Background: Whole-exome sequencing (WES) finds a CKD-related mutation in approximately 20% of patients presenting with CKD before 25 years of age. Although provision of a molecular diagnosis could have important implications for clinical management, evidence is lacking on the diagnostic yield and clinical utility of WES for pediatric renal transplant recipients.
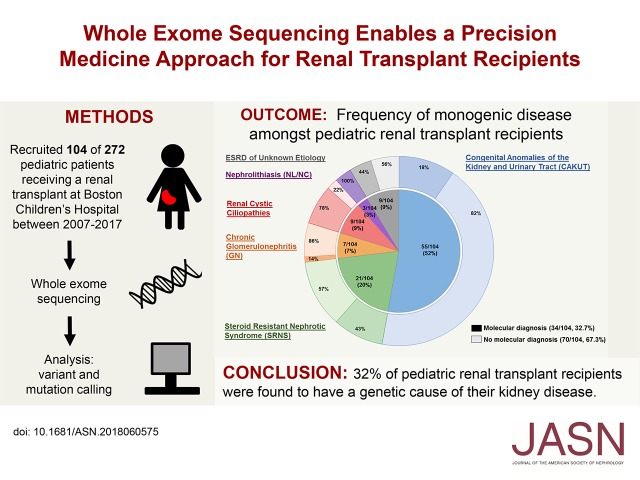
Methods: To determine the diagnostic yield of WES in pediatric kidney transplant recipients, we recruited 104 patients who had received a transplant at Boston Children's Hospital from 2007 through 2017, performed WES, and analyzed results for likely deleterious variants in approximately 400 genes known to cause CKD.
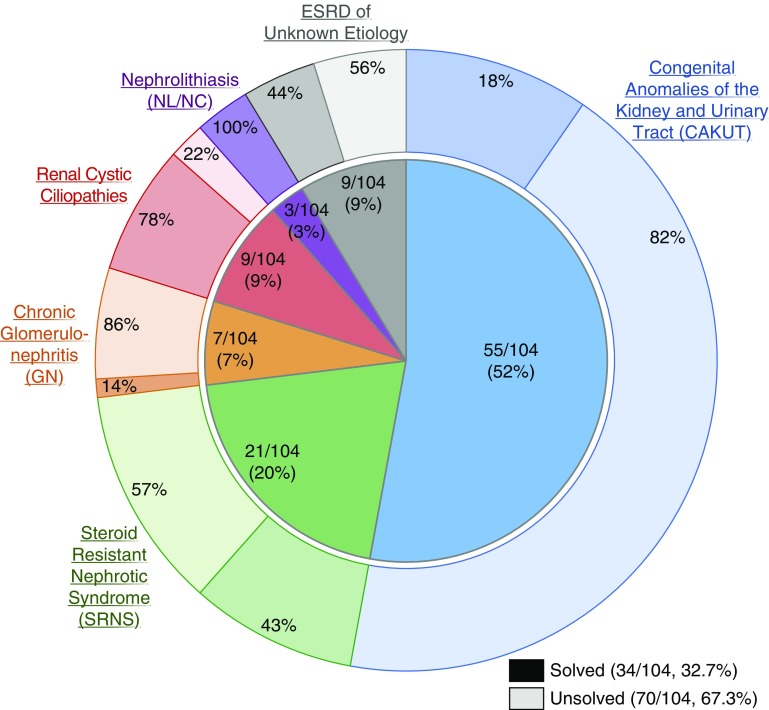
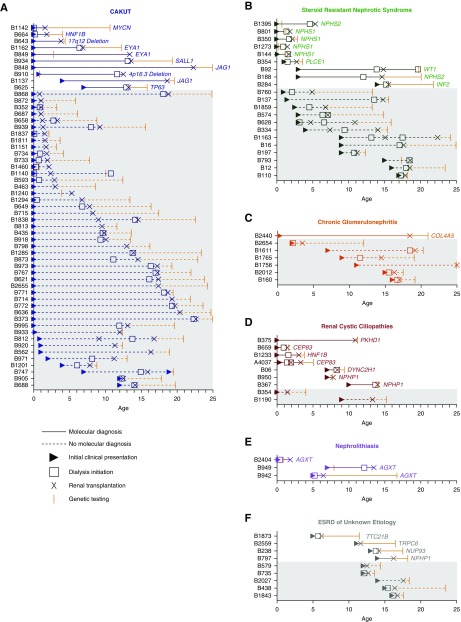
Results: By WES, we identified a genetic cause of CKD in 34 out of 104 (32.7%) transplant recipients. The likelihood of detecting a molecular genetic diagnosis was highest for patients with urinary stone disease (three out of three individuals), followed by renal cystic ciliopathies (seven out of nine individuals), steroid-resistant nephrotic syndrome (nine out of 21 individuals), congenital anomalies of the kidney and urinary tract (ten out of 55 individuals), and chronic glomerulonephritis (one out of seven individuals). WES also yielded a molecular diagnosis for four out of nine individuals with ESRD of unknown etiology. The WES-related molecular genetic diagnosis had implications for clinical care for five patients.
Conclusions: Nearly one third of pediatric renal transplant recipients had a genetic cause of their kidney disease identified by WES. Knowledge of this genetic information can help guide management of both transplant patients and potential living related donors.
Keywords: chronic kidney disease; end-stage renal disease; genetic renal disease; human genetics; transplantation.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- North American Pediatric Renal Trials and Collaborative Studies: NAPRTCS Annual Transplant Report, 2014. Available at: https://web.emmes.com/study/ped/annlrept/annualrept2014.pdf. Accessed May 1, 2018
-
- Weber S, Moriniere V, Knüppel T, Charbit M, Dusek J, Ghiggeri GM, et al. .: Prevalence of mutations in renal developmental genes in children with renal hypodysplasia: Results of the ESCAPE study. J Am Soc Nephrol 17: 2864–2870, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
