

Acute Tocolysis - a Critical Analysis of Evidence-Based Data
- PMID: 30655648
- PMCID: PMC6294642
- DOI: 10.1055/a-0717-5329
Acute Tocolysis - a Critical Analysis of Evidence-Based Data
Abstract
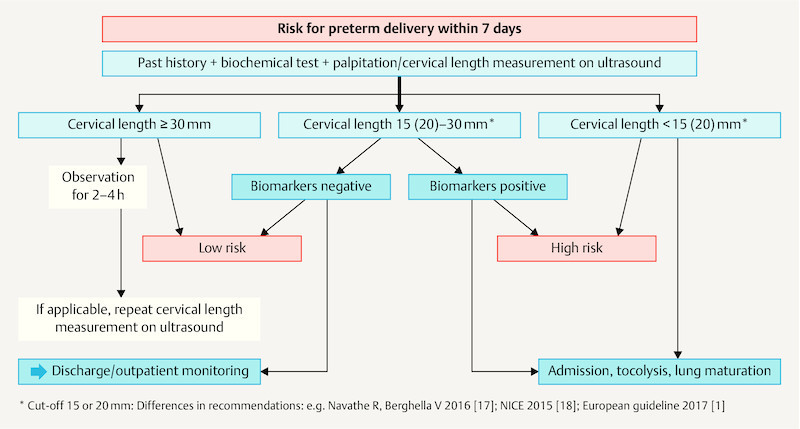
Tocolysis is among the most common obstetric measures. The objective is to prolong the pregnancy by at least 48 hours to complete foetal lung maturation and for the in-utero transfer of the pregnant woman to a perinatal centre. The indication for tocolysis is regular, premature contractions (≥ 4/20 min) and a dynamic shortening of the cervical length/cervical opening between 22 + 0 to 33 + 6 weeks of pregnancy. In this connection, the cervical length measured on ultrasound and the determination of biomarkers in the cervicovaginal secretions can be important decision-making aids. Beta sympathomimetics should no longer be used due to the high rate of severe maternal adverse effects. Given controversial data, magnesium sulphate is no longer recommended for tocolysis in current guidelines. Atosiban is as effective for prolonging pregnancy as beta sympathomimetics and nifedipine, has the lowest rate of maternal adverse effects, but also the highest drug costs. Nifedipine and indomethacin are recommended in international guidelines for acute tocolysis, however there are indications of increased neonatal morbidity following indomethacin. Current problems are, above all, the lack of randomised, controlled comparative and placebo-controlled studies, the data which are controversial to some extent, and the insufficient evidence of tocolytics to significantly improve the neonatal outcome.
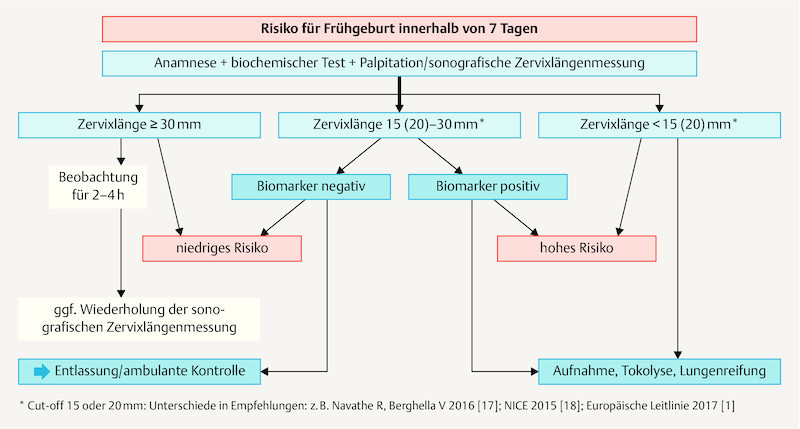
Die Tokolyse gehört zu den häufigsten geburtshilflichen Maßnahmen. Ziel ist die Verlängerung der Schwangerschaft um mindestens 48 Stunden zum Abschluss der fetalen Lungenreifung und zum In-utero-Transfer der Schwangeren in ein Perinatalzentrum. Die Indikation zur Tokolyse sind regelmäßige, vorzeitige Wehen (≥ 4/20 min) und eine dynamische Verkürzung der Zervixlänge/Zervixeröffnung zwischen 22 + 0 bis 33 + 6 SSW. In diesem Zusammenhang können die sonografisch gemessene Zervixlänge und die Bestimmung von Biomarkern im Zervikovaginalsekret wichtige Entscheidungshilfen sein. Betasympathomimetika sollten aufgrund der hohen Rate schwerer maternaler Nebenwirkungen nicht mehr eingesetzt werden. Bei kontroverser Datenlage wird Magnesiumsulfat in aktuellen Leitlinien nicht mehr zur Tokolyse empfohlen. Atosiban ist zur Schwangerschaftsverlängerung äquieffektiv zu Betasympathomimetika und Nifedipin, weist die geringste Rate maternaler Nebenwirkungen, aber auch die höchsten Arzneimittelkosten auf. Nifedipin und Indometacin werden in internationalen Leitlinien zur Akuttokolyse empfohlen, allerdings bestehen Hinweise für eine erhöhte neonatale Morbidität nach Indometacin. Derzeitige Probleme sind vor allem das Fehlen randomisierter, kontrollierter Vergleichs- und placebokontrollierter Studien, die z. T. kontroverse Datenlage und die unzureichende Evidenz von Tokolytika, das neonatale Outcome signifikant zu verbessern.
Keywords: evidence; indication and objectives; preterm contractions; safety profile; tocolysis; tocolytics.
Conflict of interest statement
Figures
Similar articles
-
[Tocolysis for preterm labor without premature preterm rupture of membranes].J Gynecol Obstet Biol Reprod (Paris). 2016 Dec;45(10):1374-1398. doi: 10.1016/j.jgyn.2016.09.018. Epub 2016 Oct 28. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 28029463 Review. French.
-
Nifedipine versus atosiban in the treatment of threatened preterm labour (Assessment of Perinatal Outcome after Specific Tocolysis in Early Labour: APOSTEL III-Trial).BMC Pregnancy Childbirth. 2014 Mar 3;14:93. doi: 10.1186/1471-2393-14-93. BMC Pregnancy Childbirth. 2014. PMID: 24589124 Free PMC article. Clinical Trial.
-
Do obstetric units adhere to the evidence-based national guideline? A Germany-wide survey on the current practice of initial tocolysis.Eur J Obstet Gynecol Reprod Biol. 2022 Mar;270:133-138. doi: 10.1016/j.ejogrb.2022.01.006. Epub 2022 Jan 10. Eur J Obstet Gynecol Reprod Biol. 2022. PMID: 35051825
-
[Prevention of spontaneous preterm birth (excluding preterm premature rupture of membranes): Guidelines for clinical practice - Text of the Guidelines (short text)].J Gynecol Obstet Biol Reprod (Paris). 2016 Dec;45(10):1446-1456. doi: 10.1016/j.jgyn.2016.09.011. Epub 2016 Nov 9. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27836377 Review. French.
-
Nifedipine versus placebo in the treatment of preterm prelabor rupture of membranes: a randomized controlled trial: Assessment of perinatal outcome by use of tocolysis in early labor-APOSTEL IV trial.Eur J Obstet Gynecol Reprod Biol. 2016 Oct;205:79-84. doi: 10.1016/j.ejogrb.2016.08.024. Epub 2016 Aug 9. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27567363 Clinical Trial.
Cited by
-
Progesterone for the Prevention of Preterm Birth - an Update of Evidence-Based Indications.Geburtshilfe Frauenheilkd. 2019 Aug;79(8):844-853. doi: 10.1055/a-0854-6472. Epub 2019 Aug 12. Geburtshilfe Frauenheilkd. 2019. PMID: 31423019 Free PMC article.
-
Progesterone - Effective for Tocolysis and Maintenance Treatment After Arrested Preterm Labour?: Critical Analysis of the Evidence.Geburtshilfe Frauenheilkd. 2019 Aug;79(8):834-843. doi: 10.1055/a-0829-3992. Epub 2019 May 13. Geburtshilfe Frauenheilkd. 2019. PMID: 31423018 Free PMC article.
-
The combined uterorelaxant effect of sildenafil and terbutalin in the rat: The potential benefit of co-administration of low doses.Heliyon. 2023 Nov 17;9(12):e22488. doi: 10.1016/j.heliyon.2023.e22488. eCollection 2023 Dec. Heliyon. 2023. PMID: 38046168 Free PMC article.
-
Tocolytic Treatment for the Prevention of Preterm Birth from a Taiwanese Perspective: A Survey of Taiwanese Obstetric Specialists.Int J Environ Res Public Health. 2022 Apr 1;19(7):4222. doi: 10.3390/ijerph19074222. Int J Environ Res Public Health. 2022. PMID: 35409902 Free PMC article.
-
Differences between Current Clinical Practice and Evidence-Based Guideline Recommendations Regarding Tocolysis - an Austria-wide Survey.Geburtshilfe Frauenheilkd. 2024 Nov 28;85(1):47-55. doi: 10.1055/a-2446-1828. eCollection 2025 Jan. Geburtshilfe Frauenheilkd. 2024. PMID: 39758118 Free PMC article.
References
-
- De Renzo G C, Roura L C, Facchinetti F. Preterm labor and birth management: Recommendations from the European Association of Perinatal Medicine. J Matern Fetal Neonatal Med. 2017;30:2011–2030. - PubMed
-
- IQTIG Institut für Qualitätssicherung und Transparenz im Gesundheitswesen 2018. Basisauswertung zum Erfassungsjahr 2017: GeburtshilfeOnline:https://iqtig.org/downloads/auswertung/2017/16n1gebh/QSKH_16n1-GEBH_2017...last access: 01.08.2018
-
- ACOG . Practice Bulletin No. 171. Management of preterm labour. Obstet Gynecol. 2016;128:e155–e164. - PubMed
-
- Hackney D N, Olson-Chen C, Thomberg L L. What do we know above the natural outcomes of preterm labour? A systematic review and meta-analysis of women without tocolysis in preterm labour. Paediatr Perinat Epidemiol. 2013;27:452–460. - PubMed
-
- Nijman T AJ, van Vliet E OG, Koullali B. Antepartum and intrapartum interventions to prevent preterm birth and its sequelae. Semin Fetal Neonatal Med. 2016;21:121–128. - PubMed
LinkOut - more resources
Full Text Sources