

Extracellular matrix differences in glioblastoma patients with different prognoses
- PMID: 30655832
- PMCID: PMC6313004
- DOI: 10.3892/ol.2018.9649
Extracellular matrix differences in glioblastoma patients with different prognoses
Abstract
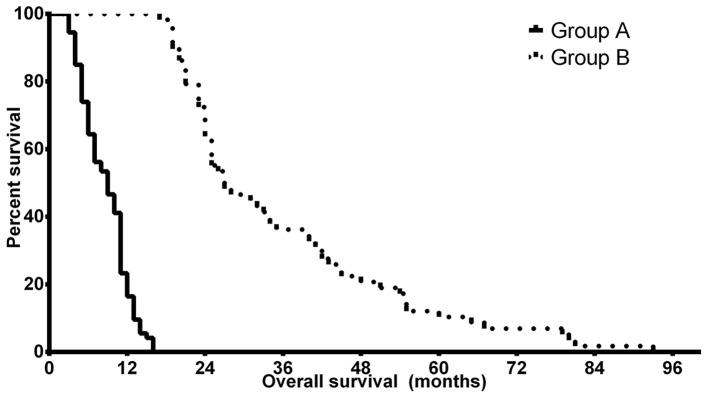
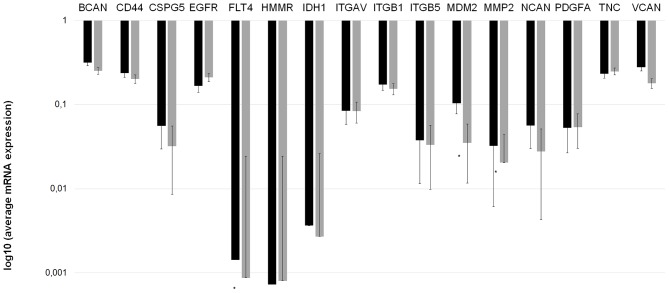
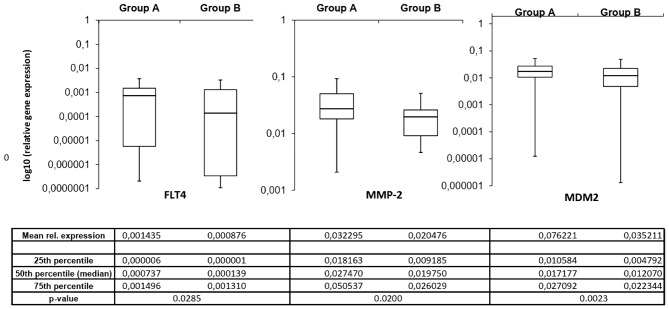
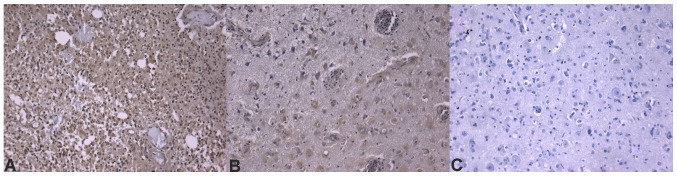
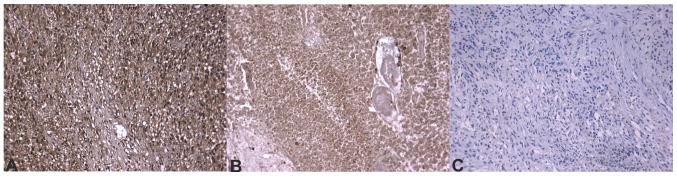
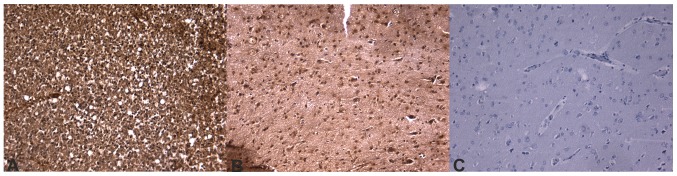
Glioblastoma is the most common malignant central nervous system tumor. Patient outcome remains poor despite the development of therapy and increased understanding of the disease in the past decades. Glioma cells invade the peritumoral brain, which results in inevitable tumor recurrence. Previous studies have demonstrated that the extracellular matrix (ECM) is altered in gliomas and serves a major role in glioma invasion. The present study focuses on differences in the ECM composition of tumors in patients with poor and improved prognosis. The mRNA and protein expression of 16 invasion-associated ECM molecules was determined using reverse trascription-quantitiative polymerase chain reaction and immunohistochemistry, respectively. Clinical factors of patients with different prognoses was also analyzed. It was determined that age and postoperative Karnofsky performance score were associated with patient survival. Furthermore, Fms-related tyrosine kinase 4/vascular endothelial growth factor receptor 3 (FLT4/VEGFR3), murine double minute 2 (MDM2) and matrix metallopeptidase 2 (MMP2) mRNA levels were significantly different between the two prognostic groups. Additionally, brevican, cluster of differentiation 44, hyaluronan mediated motility receptor, integrin-αV and -β1, and MDM2 protein expression were indicated to be significantly different in immunohistochemistry slides. Using the expression profile, including the invasion spectrum of the samples, it was possible to identify the prognostic group of the sample with high efficacy, particularly in cases with poor prognosis. In conclusion, it was determined that ECM components exhibit different expression levels in tumors with different prognoses and thus the invasion spectrum can be used as a prognostic factor in glioblastoma.
Keywords: expression; extracellular matrix; glioblastoma; prognosis; survival.
Figures
Similar articles
-
Prognostic Role of the Expression of Invasion-Related Molecules in Glioblastoma.J Neurol Surg A Cent Eur Neurosurg. 2017 Jan;78(1):12-19. doi: 10.1055/s-0036-1584920. Epub 2016 Aug 16. J Neurol Surg A Cent Eur Neurosurg. 2017. PMID: 27529670
-
Expression of invasion-related extracellular matrix molecules in human glioblastoma versus intracerebral lung adenocarcinoma metastasis.Cent Eur Neurosurg. 2010 Nov;71(4):173-80. doi: 10.1055/s-0030-1249698. Epub 2010 Apr 15. Cent Eur Neurosurg. 2010. PMID: 20397122
-
Tumor Grade versus Expression of Invasion-Related Molecules in Astrocytoma.Pathol Oncol Res. 2018 Jan;24(1):35-43. doi: 10.1007/s12253-017-0194-6. Epub 2017 Feb 4. Pathol Oncol Res. 2018. PMID: 28161812
-
Microregional extracellular matrix heterogeneity in brain modulates glioma cell invasion.Int J Biochem Cell Biol. 2004 Jun;36(6):1046-69. doi: 10.1016/j.biocel.2004.01.013. Int J Biochem Cell Biol. 2004. PMID: 15094120 Review.
-
Glial tumor invasion: a role for the upregulation and cleavage of BEHAB/brevican.Neuroscientist. 2001 Apr;7(2):113-22. doi: 10.1177/107385840100700206. Neuroscientist. 2001. PMID: 11496922 Review.
Cited by
-
Tumor Cell Infiltration into the Brain in Glioblastoma: From Mechanisms to Clinical Perspectives.Cancers (Basel). 2022 Jan 17;14(2):443. doi: 10.3390/cancers14020443. Cancers (Basel). 2022. PMID: 35053605 Free PMC article. Review.
-
Microphysiological systems to study tumor-stroma interactions in brain cancer.Brain Res Bull. 2021 Sep;174:220-229. doi: 10.1016/j.brainresbull.2021.06.012. Epub 2021 Jun 21. Brain Res Bull. 2021. PMID: 34166771 Free PMC article. Review.
-
Targeting Glioblastoma Tumor Microenvironment.Adv Exp Med Biol. 2020;1296:1-9. doi: 10.1007/978-3-030-59038-3_1. Adv Exp Med Biol. 2020. PMID: 34185283 Review.
-
High VEGFA Expression Is Associated with Improved Progression-Free Survival after Bevacizumab Treatment in Recurrent Glioblastoma.Cancers (Basel). 2023 Apr 7;15(8):2196. doi: 10.3390/cancers15082196. Cancers (Basel). 2023. PMID: 37190125 Free PMC article.
-
Overcoming Resistance to Temozolomide in Glioblastoma: A Scoping Review of Preclinical and Clinical Data.Life (Basel). 2024 May 24;14(6):673. doi: 10.3390/life14060673. Life (Basel). 2024. PMID: 38929657 Free PMC article.
References
-
- Grossman SA, Ye X, Piantadosi S, Desideri S, Nabors LB, Rosenfeld M, Fisher J NABTT CNS Consortium, corp-author. Survival of patients with newly diagnosed glioblastoma treated with radiation and temozolomide in research studies in the United States. Clin Cancer Res. 2010;16:2443–2449. doi: 10.1158/1078-0432.CCR-09-3106. - DOI - PMC - PubMed
-
- Back MF, Ang ELL, Ng WH, See SJ, Lim CCT, Chan SP, Yeo TT. Improved median survival for glioblastoma multiforme following introduction of adjuvant temozolomide chemotherapy. Ann Acad Med Singapore. 2007;36:338–342. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous