

Comparisons of Submental and Groin Vascularized Lymph Node Flaps Transfer for Breast Cancer-Related Lymphedema
- PMID: 30656093
- PMCID: PMC6326621
- DOI: 10.1097/GOX.0000000000001923
Comparisons of Submental and Groin Vascularized Lymph Node Flaps Transfer for Breast Cancer-Related Lymphedema
Abstract
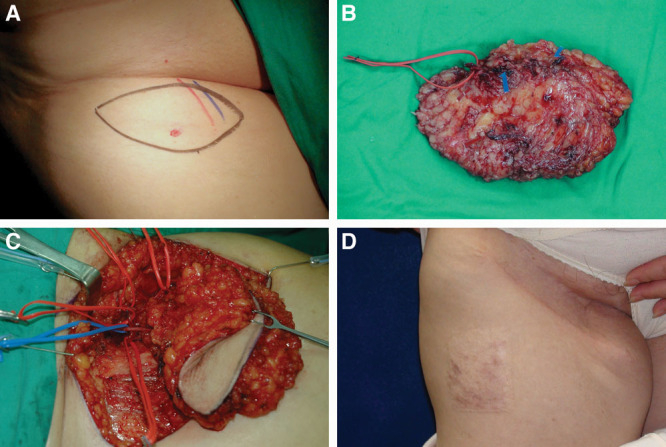
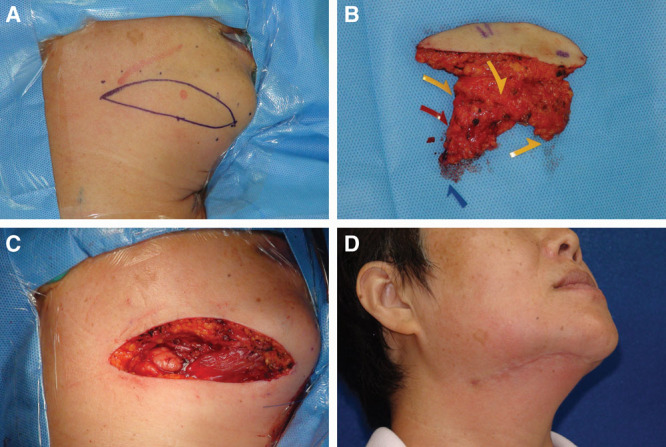
Background: The vascularized groin and submental lymph node (VGLN and VSLN) flaps are valuable options in the treatment of lymphedema. This study was to compare outcomes between VGLN and VSLN transfers for breast cancer-related lymphedema.
Methods: Between January 2008 and December 2016, VGLN and VSLN transfers for upper limb lymphedema were compared including flap characteristics, flap elevation time, complications, and limb circumference changes.
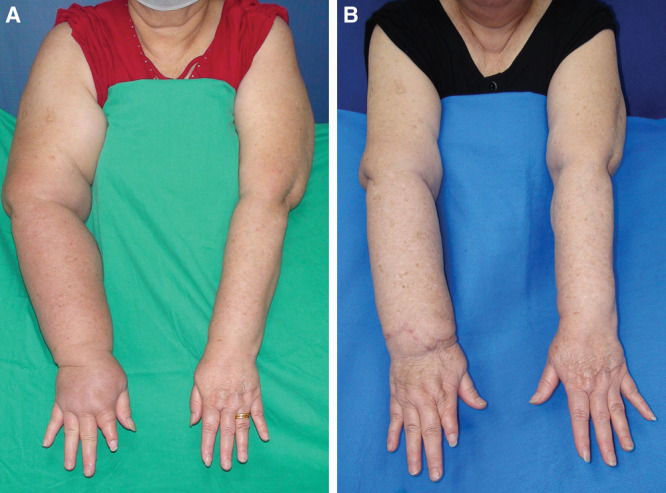
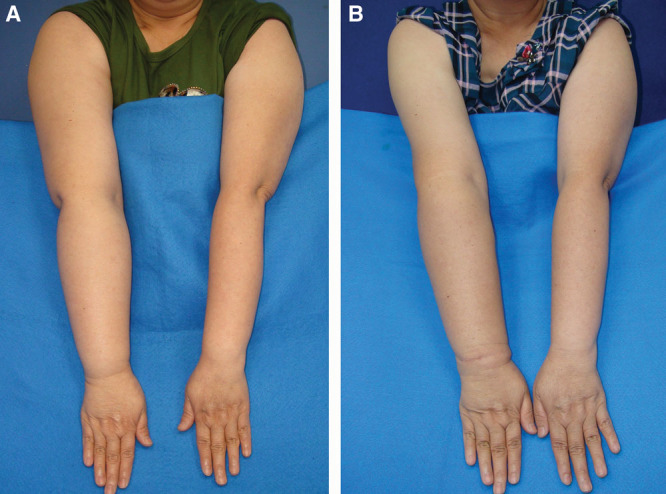
Results: All flaps survived. Similar vein (2.6 versus 3.2 mm; P = 0.3) and artery diameter (2.1 versus 2.8 mm; P = 0.3) and number of lymph nodes (3 versus 4; P = 0.4) were found between VGLN and VSLN groups, respectively. Circumferential reduction rate was higher in VSLN than VGLN (P = 0.04) group. Vascular complication rate with salvage rate was not statistically different between the 2 groups. Donor-site complication and total complication rates were statistically higher in VGLN than VSLN flaps (7.7% versus 0%, P = 0.004; 46.2% versus 23.3%, P = 0.002). At a mean 39.8 ± 22.4 months, the circumferential reduction rate was statistically higher in VSLN than in the VGLN group (55.5 ± 14.3% versus 48.4 ± 23.9%, P = 0.04). Both flaps were effectively decreased in the episodes of cellulitis.
Conclusions: Both VGLN and VSLN flaps are valuable surgical options in treating breast cancer-related lymphedema. However, the VSLN flap for breast cancer-related lymphedema is better in providing more significant improvements in limb circumference, a faster flap harvest time, decreased complication rates, and minimal donor-site iatrogenic lymphedema.
Figures
References
-
- Campisi C, Bellini C, Accogli S, et al. Microsurgery for lymphedema: clinical research and long-term results. Microsurgery. 2010;30:256. - PubMed
-
- Chang DW. Lymphaticovenular bypass for lymphedema management in breast cancer patients: a prospective study. Plast Reconstr Surg. 2010;126:752. - PubMed
-
- Koshima I, Nanba Y, Tsutsui T, et al. Minimal invasive lymphaticovenular anastomosis under local anesthesia for leg lymphedema: is it effective for stage III and IV? Ann Plast Surg. 2004;53:261. - PubMed
-
- Cheng MH, Chang DW, Patel KM. Principles and Practice of Lymphedema Surgery. 2016Oxford, UK: Elsevier.
LinkOut - more resources
Full Text Sources