

IVIg-induced plasmablasts in patients with Guillain-Barré syndrome
- PMID: 30656191
- PMCID: PMC6331722
- DOI: 10.1002/acn3.687
IVIg-induced plasmablasts in patients with Guillain-Barré syndrome
Abstract
Objective: The Guillain-Barré syndrome (GBS) is an acute, immune-mediated disease of peripheral nerves. Plasmablasts and plasma cells play a central role in GBS by producing neurotoxic antibodies. The standard treatment for GBS is high-dose intravenous immunoglobulins (IVIg), however the working mechanism is unknown and the response to treatment is highly variable. We aimed to determine whether IVIg changes the frequency of B-cell subsets in patients with GBS.
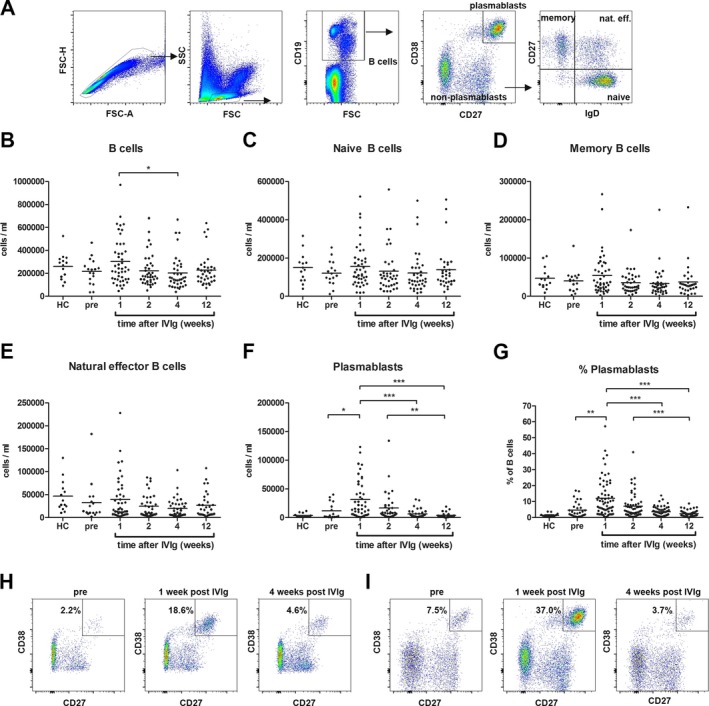
Methods: Peripheral blood mononuclear cells were isolated from 67 patients with GBS before and/or 1, 2, 4, and 12 weeks after treatment with high-dose IVIg. B-cell subset frequencies were determined by flow cytometry and related to serum immunoglobulin levels. Immunoglobulin transcripts before and after IVIg treatment were examined by next-generation sequencing. Antiglycolipid antibodies were determined by ELISA.
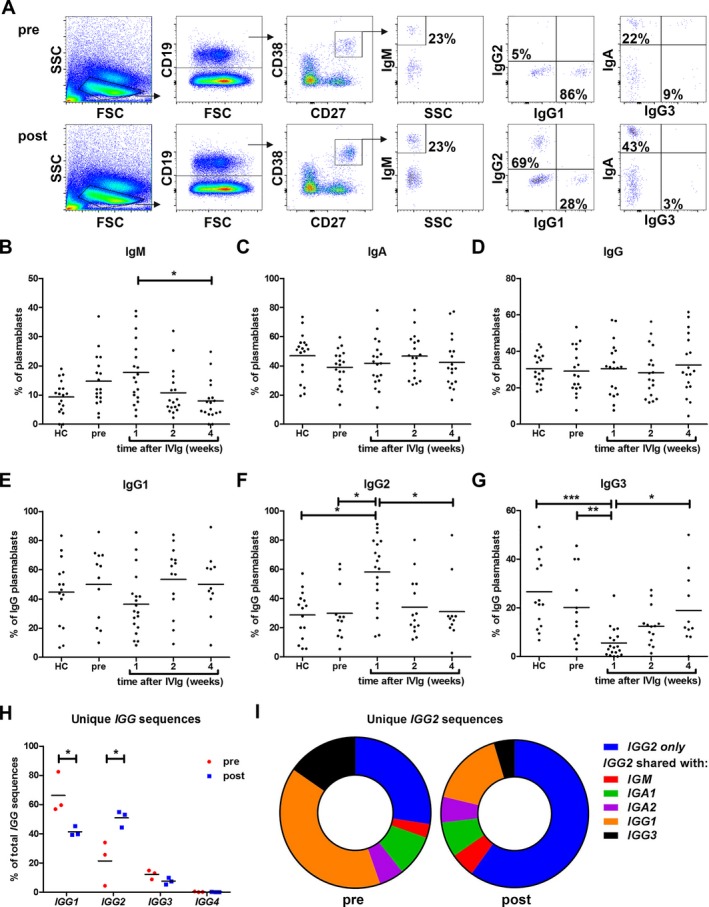
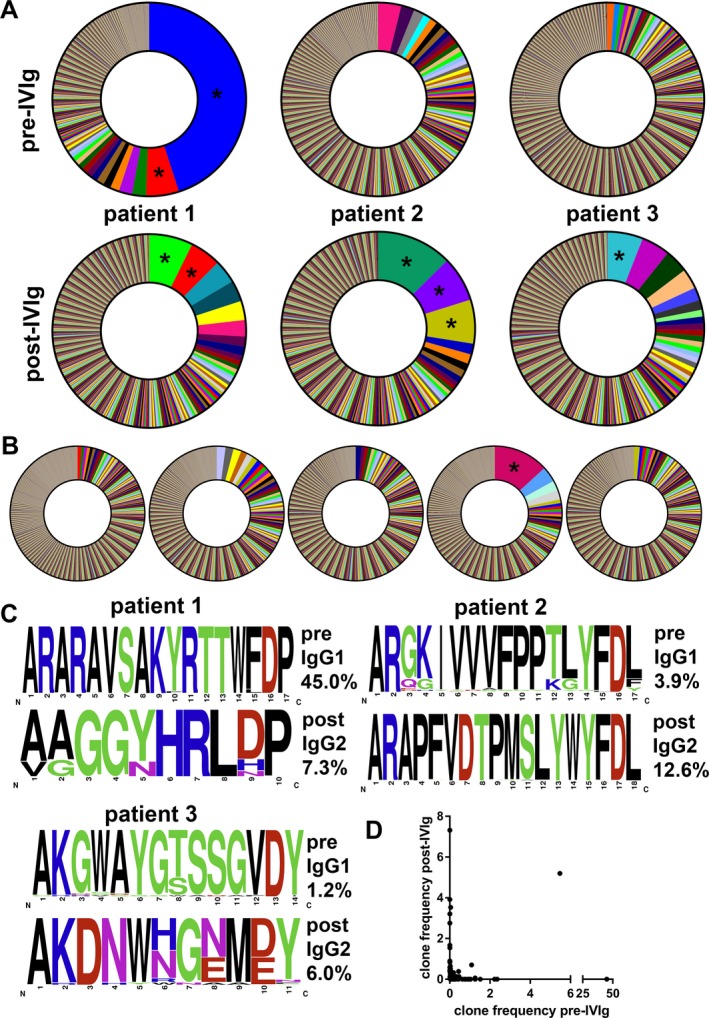
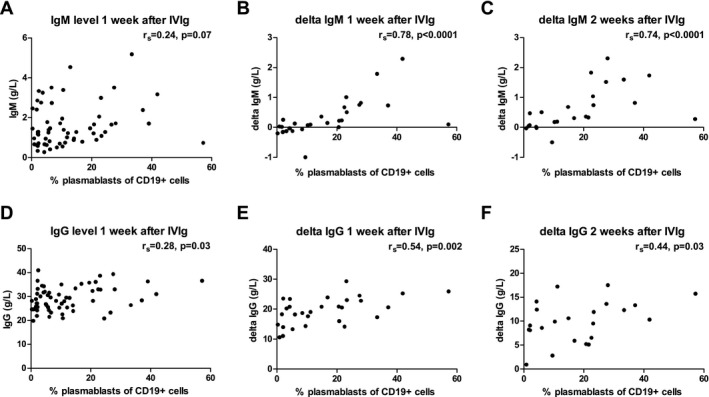
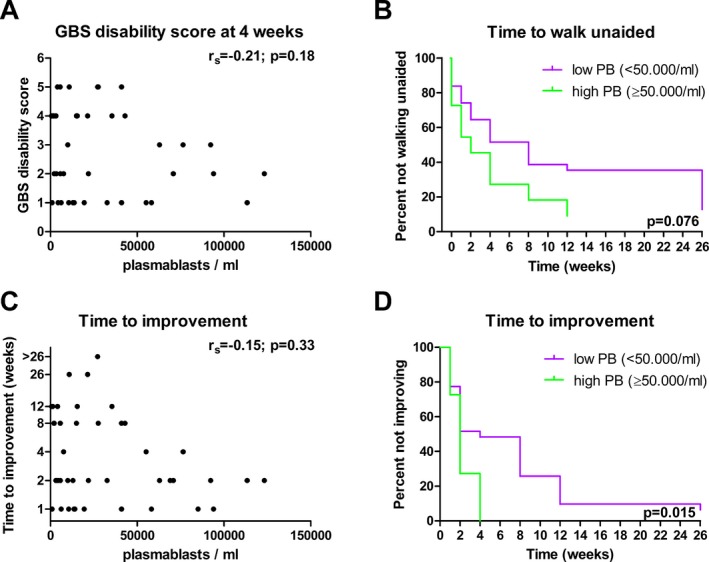
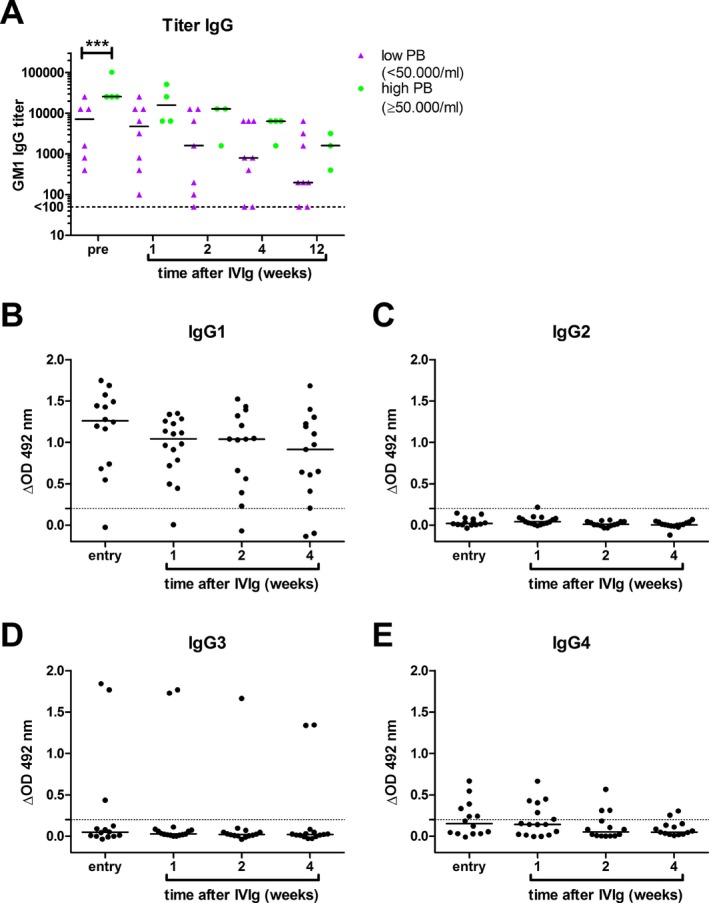
Results: Patients treated with IVIg demonstrated a strong increase in plasmablasts, which peaked 1 week after treatment. Flow cytometry identified a relative increase in IgG2 plasmablasts posttreatment. Within IGG sequences, dominant clones were identified which were also IGG2 and had different immunoglobulin sequences compared to pretreatment samples. High plasmablast frequencies after treatment correlated with an increase in serum IgG and IgM, suggesting endogenous production. Patients with a high number of plasmablasts started to improve earlier (P = 0.015) and were treated with a higher dose of IVIg.
Interpretation: High-dose IVIg treatment alters the distribution of B-cell subsets in the peripheral blood of GBS patients, suggesting de novo (oligo-)clonal B-cell activation. Very high numbers of plasmablasts after IVIg therapy may be a potential biomarker for fast clinical recovery.
Figures
Similar articles
-
IgG Fc N-glycosylation in Guillain-Barré syndrome treated with immunoglobulins.J Proteome Res. 2014 Mar 7;13(3):1722-30. doi: 10.1021/pr401213z. Epub 2014 Feb 17. J Proteome Res. 2014. PMID: 24533874 Clinical Trial.
-
Changes of Serum IgG Dimer Levels after Treatment with IVIg in Guillain-Barré Syndrome.J Neuroimmune Pharmacol. 2019 Dec;14(4):642-648. doi: 10.1007/s11481-019-09871-0. Epub 2019 Sep 12. J Neuroimmune Pharmacol. 2019. PMID: 31515689
-
Intravenous immunoglobulins neutralize blocking antibodies in Guillain-Barré syndrome.Ann Neurol. 2002 Jun;51(6):673-80. doi: 10.1002/ana.10205. Ann Neurol. 2002. PMID: 12112071
-
IVIG treatment and prognosis in Guillain-Barré syndrome.J Clin Immunol. 2010 May;30 Suppl 1(Suppl 1):S74-8. doi: 10.1007/s10875-010-9407-4. J Clin Immunol. 2010. PMID: 20396937 Free PMC article. Review.
-
Diagnosis, treatment and prognosis of Guillain-Barré syndrome (GBS).Presse Med. 2013 Jun;42(6 Pt 2):e193-201. doi: 10.1016/j.lpm.2013.02.328. Epub 2013 Apr 28. Presse Med. 2013. PMID: 23628447 Review.
Cited by
-
High-Dose Intravenous Immunoglobulins in the Treatment of Severe Acute Viral Pneumonia: The Known Mechanisms and Clinical Effects.Front Immunol. 2020 Jul 14;11:1660. doi: 10.3389/fimmu.2020.01660. eCollection 2020. Front Immunol. 2020. PMID: 32760407 Free PMC article. Review.
-
Neutrophil-to-lymphocyte ratio is a risk indicator of Guillain-Barré syndrome and is associated with severity and short-term prognosis.Heliyon. 2023 Mar 10;9(3):e14321. doi: 10.1016/j.heliyon.2023.e14321. eCollection 2023 Mar. Heliyon. 2023. PMID: 36967912 Free PMC article.
-
Guillain-Barré syndrome: expanding the concept of molecular mimicry.Trends Immunol. 2022 Apr;43(4):296-308. doi: 10.1016/j.it.2022.02.003. Epub 2022 Mar 4. Trends Immunol. 2022. PMID: 35256276 Free PMC article. Review.
-
B Cells and Antibodies as Targets of Therapeutic Intervention in Neuromyelitis Optica Spectrum Disorders.Pharmaceuticals (Basel). 2021 Jan 6;14(1):37. doi: 10.3390/ph14010037. Pharmaceuticals (Basel). 2021. PMID: 33419217 Free PMC article. Review.
-
A Case of Type 2 Diabetes Mellitus Revealed Transient Positivity of Glutamic Acid Decarboxylase (GAD) Antibodies Following Immunoglobulin Administrations.Cureus. 2024 Aug 9;16(8):e66485. doi: 10.7759/cureus.66485. eCollection 2024 Aug. Cureus. 2024. PMID: 39247010 Free PMC article.
References
-
- Willison HJ, Jacobs BC, van Doorn PA. Guillain‐Barré syndrome. Lancet 2016;388:717–727. - PubMed
-
- McGonigal R, Rowan EG, Greenshields KN, et al. Anti‐GD1a antibodies activate complement and calpain to injure distal motor nodes of Ranvier in mice. Brain 2010;133:1944–1960. - PubMed
-
- van der Meché FG, Schmitz PI. A randomized trial comparing intravenous immune globulin and plasma exchange in Guillain‐Barré syndrome. Dutch Guillain‐Barré Study Group. N Engl J Med 1992;326:1123–1129. - PubMed
-
- van Doorn PA, Ruts L, Jacobs BC. Clinical features, pathogenesis, and treatment of Guillain‐Barré syndrome. Lancet Neurol 2008;7:939–950. - PubMed
-
- Kuitwaard K, de Gelder J, Tio‐Gillen AP, et al. Pharmacokinetics of intravenous immunoglobulin and outcome in Guillain‐Barré syndrome. Ann Neurol 2009;66:597–603. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
