

Pilomotor seizures marked by infraslow activity and acetazolamide responsiveness
- PMID: 30656195
- PMCID: PMC6331207
- DOI: 10.1002/acn3.695
Pilomotor seizures marked by infraslow activity and acetazolamide responsiveness
Abstract
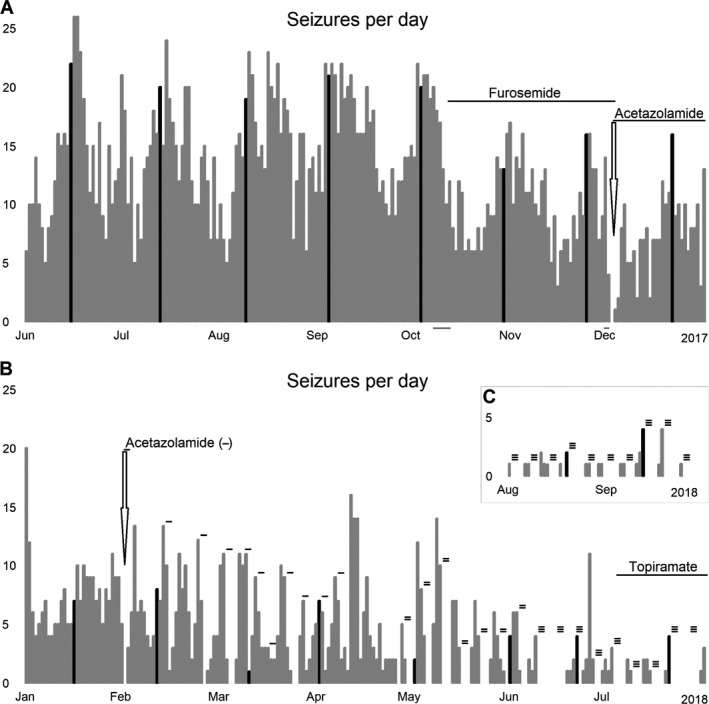
A patient with pilomotor seizures post anti-LGI1 limbic encephalitis, refractory to immunotherapy and anti-epileptic drugs, was investigated with electroencephalography and magnetoencephalography. Seizures occurred daily (14.9 ± 4.9/day), with catamenial exacerbation, inducible by hyperventilation. Anterior temporal ictal onsets were heralded (by ~15 sec) by high amplitude ipsilateral electromagnetic infraslow activity. The catamenial/ventilatory sensitivity and the infraslow activity (reflecting glial depolarization) suggested an ionic, CO 2/pH-related glioneuronal mechanism. Furosemide decreased seizure frequency by ~33%. Acetazolamide led to immediate seizure freedom, but lost efficacy with daily treatment. A cycling acetazolamide regimen (2 days on, 4 days off) plus low-dose topiramate maintained >95% reduction (0.5 ± 0.9/day) in seizures.
Figures


Similar articles
-
Acetazolamide as an effective treatment for pilomotor seizures in autoimmune encephalitis.Epilepsia. 2024 May;65(5):e67-e72. doi: 10.1111/epi.17962. Epub 2024 Mar 27. Epilepsia. 2024. PMID: 38536044
-
[Ictal electroencephalography (EEG) activity and cerebral blood flow dynamics as potential pathological indicators: a case of anti-leucine-rich glioma-inactivated 1 protein (LGI1) encephalitis].Rinsho Shinkeigaku. 2020 Nov 27;60(11):778-785. doi: 10.5692/clinicalneurol.cn-001460. Epub 2020 Oct 27. Rinsho Shinkeigaku. 2020. PMID: 33115994 Japanese.
-
Seizure semiology in leucine-rich glioma-inactivated protein 1 antibody-associated limbic encephalitis.Epilepsy Behav. 2017 Dec;77:90-95. doi: 10.1016/j.yebeh.2017.08.011. Epub 2017 Oct 17. Epilepsy Behav. 2017. PMID: 29050866
-
Pilomotor seizures in autoimmune limbic encephalitis: description of two GAD65 antibodies- related cases and literature review.Seizure. 2022 May;98:71-78. doi: 10.1016/j.seizure.2022.03.025. Epub 2022 Apr 5. Seizure. 2022. PMID: 35427850 Review.
-
Status-like recurrent pilomotor seizures: case report and review of the literature.J Neurol Neurosurg Psychiatry. 2000 May;68(5):647-9. doi: 10.1136/jnnp.68.5.647. J Neurol Neurosurg Psychiatry. 2000. PMID: 10766899 Free PMC article. Review.
Cited by
-
Hyperventilation-induced focal seizures in adults: think autoimmune encephalitis.Ann Clin Transl Neurol. 2022 Jun;9(6):877-881. doi: 10.1002/acn3.51566. Epub 2022 Apr 30. Ann Clin Transl Neurol. 2022. PMID: 35488768 Free PMC article.
References
-
- Irani S, Michell AW, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol 2011;69:892–900. - PubMed
-
- Navarro V, Kas A, Apartis E, et al. Motor cortex and hippocampus are the two main cortical targets in LGI1‐antibody encephalitis. Brain 2016;139:1079–1093. - PubMed
-
- Wennberg R, Steriade C, Chen R, Andrade D. Frontal infraslow activity marks the motor spasms of anti‐LGI1 encephalitis. Clin Neurophysiol 2018;129:59–68. - PubMed
-
- Steriade C, Mirsattari SM, Murray BJ, Wennberg R. Subclinical temporal EEG seizure pattern in LGI1‐antibody—mediated encephalitis. Epilepsia 2016;57:e155–e160. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical