

Thrombotic thrombocytopenic purpura: Toward targeted therapy and precision medicine
- PMID: 30656273
- PMCID: PMC6332733
- DOI: 10.1002/rth2.12160
Thrombotic thrombocytopenic purpura: Toward targeted therapy and precision medicine
Abstract
Thrombotic thrombocytopenic purpura (TTP) is a thrombotic microangiopathy characterized by severe congenital or immune-mediated deficiency in ADAMTS13, the enzyme that cleaves von Willebrand factor multimers. This rare condition leads invariably and rapidly to a fatal outcome in the absence of treatment, and therefore raises multiple diagnostic and therapeutic challenges. The novel concepts and mechanisms identified in the laboratory for this disease have been rapidly and successfully translated into the clinic for the benefit of patients, making TTP an archetypal disease that has benefited from targeted therapies. After decades of empirical treatment with plasma exchange, identification of ADAMTS13 as the key enzyme involved in TTP pathophysiology provided an explanation for the remarkable efficacy of plasma administration, in which the missing enzyme is replenished, and paved the way for development of a recombinant form of the enzyme. Similarly, the demonstration of a major role of anti-ADAMTS13 antibodies through models of passive transfer of autoimmunity spurred development of immunomodulatory strategies based on B-cell depletion. More recently, an inhibitor of the platelet-von Willebrand factor interaction demonstrated efficacy in large clinical trials through prevention of formation of further microthrombi and protection of organs from ischemia. These translational breakthroughs in TTP are described in our review.
Keywords: ADAMTS13; caplacizumab; precision medicine; rituximab; targeted therapies; thrombotic thrombocytopenic purpura.
Figures
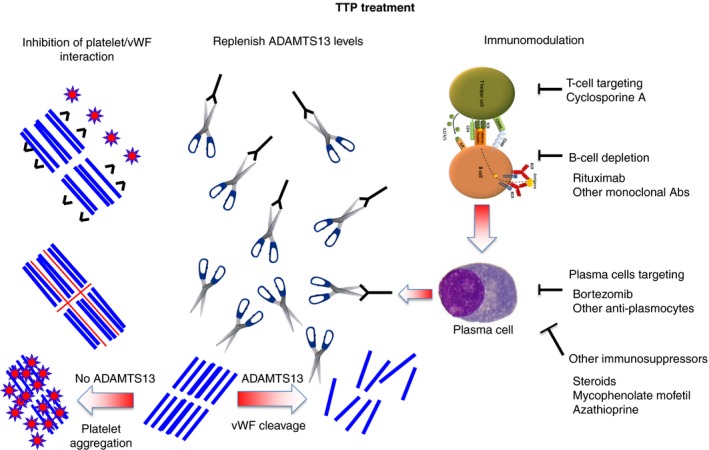
 , ADAMTS13;
, ADAMTS13;  , platelets;
, platelets;  , von Willebrand factor;
, von Willebrand factor;  , anti‐ADAMTS13 antibodies;
, anti‐ADAMTS13 antibodies;  , anti‐vWF nanobody (caplacizumab);
, anti‐vWF nanobody (caplacizumab);  , N‐acetylcysteine
, N‐acetylcysteine
References
-
- Rock GA, Shumak KH, Buskard NA, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med. 1991;325:393–7. - PubMed
-
- Furlan M, Robles R, Galbusera M, et al. von Willebrand factor‐cleaving protease in thrombotic thrombocytopenic purpura and the hemolytic‐uremic syndrome. N Engl J Med. 1998;339:1578–84. - PubMed
-
- Kremer Hovinga JA, Coppo P, Lammle B, Moake JL, Miyata T, Vanhoorelbeke K. Thrombotic thrombocytopenic purpura. Nat Rev Dis Primers. 2017;3:17020. - PubMed
-
- Joly BS, Coppo P, Veyradier A. Thrombotic thrombocytopenic purpura. Blood. 2017;129:2836–46. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
