

Circulating endothelial cells as biomarker for cardiovascular diseases
- PMID: 30656276
- PMCID: PMC6332781
- DOI: 10.1002/rth2.12158
Circulating endothelial cells as biomarker for cardiovascular diseases
Abstract
Background: Endothelial dysfunction is involved in several cardiovascular diseases. Elevated levels of circulating endothelial cells (CECs) and low levels of endothelial progenitor cells (EPCs) have been described in different cardiovascular conditions, suggesting their potential use as diagnostic biomarkers for endothelial dysfunction. Compared to typical peripheral blood leukocyte subsets, CECs and EPCs occur at very low frequency. The reliable identification and characterization of CECs and EPCs is a prerequisite for their clinical use, however, a validated method to this purpose is still missing but a key for rare cell events.
Objectives: To establish a validated flow cytometric procedure in order to quantify CECs and EPCs in human whole blood.
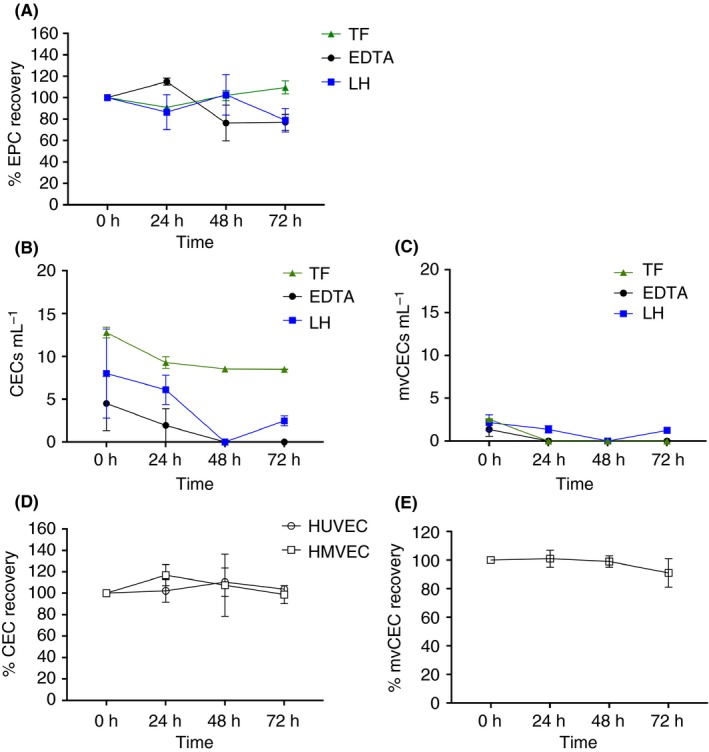
Methods: In the establishment phase, the assay sensitivity, robustness, and the sample storage conditions were optimized as prerequisite for clinical use. In a second phase, CECs and EPCs were analyzed in heart failure with preserved (HFpEF) and reduced (HFrEF) ejection fraction, in arterial hypertension (aHT), and in diabetic nephropathy (DN) in comparison to age-matched healthy controls.
Results: The quantification procedure for CECs and EPCs showed high sensitivity and reproducibility. CEC values resulted significantly increased in patients with DN and HFpEF in comparison to healthy controls. CEC quantification showed a diagnostic sensitivity of 90% and a sensitivity of 68.0%, 70.4%, and 66.7% for DN, HFpEF, and aHT, respectively.
Conclusion: A robust and precise assay to quantify CECs and EPCs in pre-clinical and clinical studies has been established. CEC counts resulted to be a good diagnostic biomarker for DN and HFpEF.
Keywords: biomarkers; cardiovascular diseases; endothelial cells; endothelial progenitor cells; flow cytometry.
Figures




References
-
- Endemann DH, Schiffrin EL. Endothelial dysfunction. J Am Soc Nephrol. 2004;15:1983–92. - PubMed
-
- Peters K, Unger RE, Brunner J, Kirkpatrick CJ. Molecular basis of endothelial dysfunction in sepsis. Cardiovasc Res. 2003;60:49–57. - PubMed
-
- Landray MJ, Wheeler DC, Lip GY, et al. Inflammation, endothelial dysfunction, and platelet activation in patients with chronic kidney disease: the chronic renal impairment in Birmingham (CRIB) study. Am J Kidney Dis. 2004;43:244–53. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
