

2D versus 3D laparoscopic total mesorectal excision: a developmental multicentre randomised controlled trial
- PMID: 30656453
- PMCID: PMC6722156
- DOI: 10.1007/s00464-018-06630-9
2D versus 3D laparoscopic total mesorectal excision: a developmental multicentre randomised controlled trial
Abstract
Aims: The role of laparoscopy in rectal cancer has been questioned. 3D laparoscopic systems are suggested to aid optimal surgical performance but have not been evaluated in advanced procedures. We hypothesised that stereoscopic imaging could improve the performance of laparoscopic total mesorectal excision (TME).
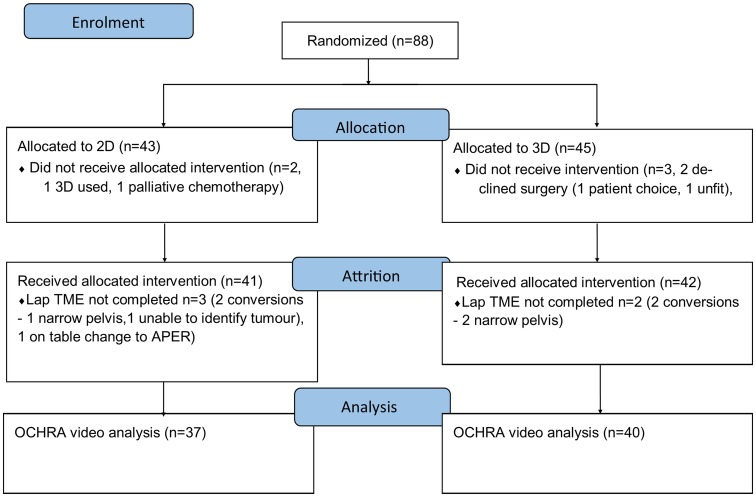
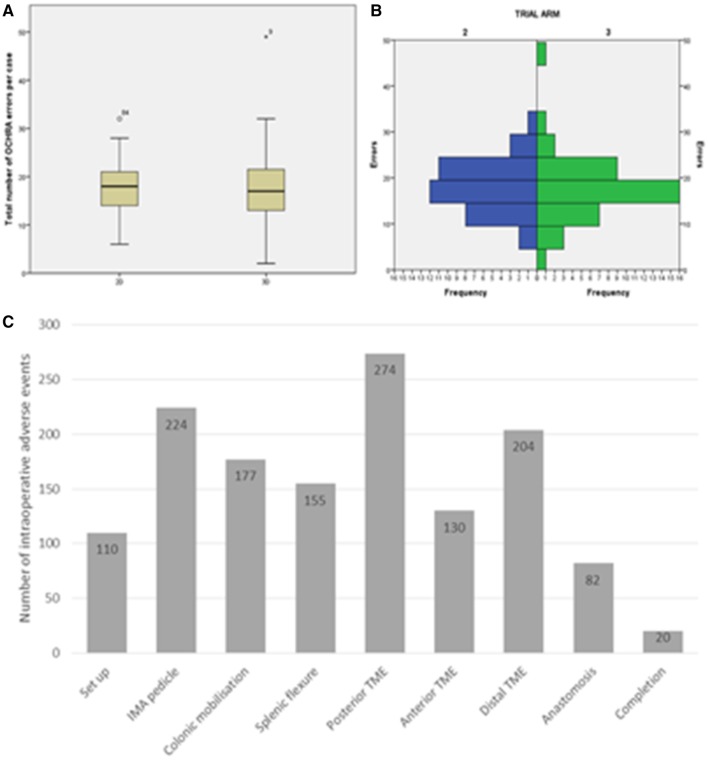
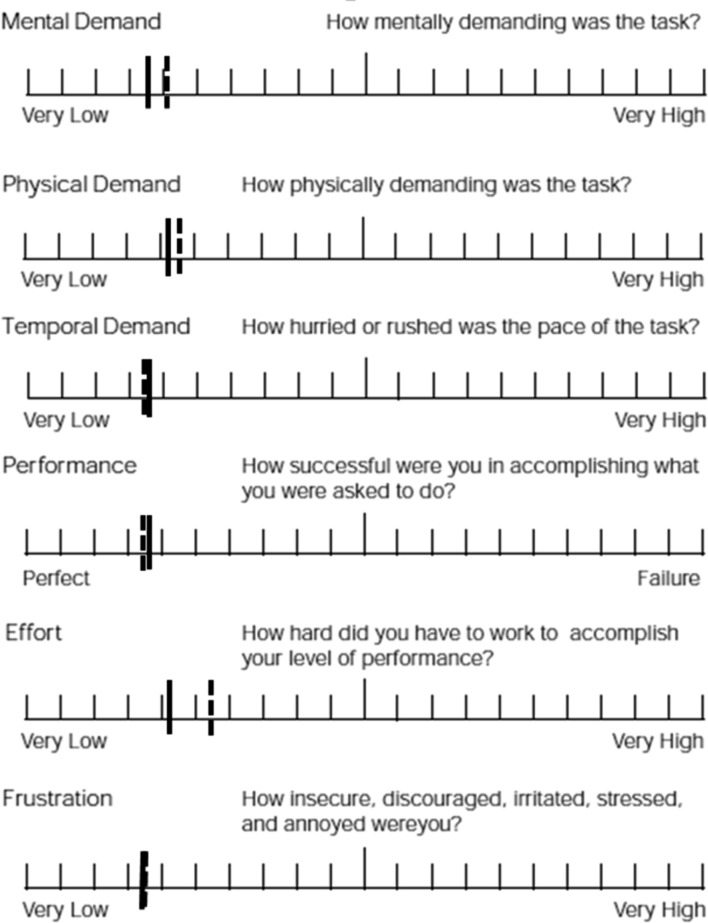
Methods: A multicentre developmental randomised controlled trial comparing 2D and 3D laparoscopic TME was performed (ISRCTN59485808). Trial surgeons were colorectal consultants that had completed their TME proficiency curve and underwent stereoscopic visual testing. Patients requiring elective laparoscopic TME with curative intent were centrally randomised (1:1) to 2D or 3D using Karl Storz IMAGE1 S D3-Link™ and 10-mm TIPCAM®1S 3D passive polarising laparoscopic systems. Outcomes were enacted adverse events as assessed by the observational clinical human reliability analysis technique, intraoperative data, 30-day patient outcomes, histopathological specimen assessment and surgeon cognitive load.
Results: 88 patients were included. There were no differences in patient or tumour demographics, surgeon stereopsis, case difficulty, cognitive load, operative time, blood loss or conversion between the trial arms. 1377 intraoperative adverse events were identified (median 18 per case, IQR 14-21, range 2-49) with no differences seen between the 2D and 3D arms (18 (95% CI 17-21) vs. 17 (95% CI 16-19), p = 0.437). 3D laparoscopy had non-significantly higher mesorectal fascial plane resections (94 vs. 77%, p = 0.059; OR 0.23 (95% CI 0.05-1.16)) but equal lymph node yield and circumferential margin distance and involvement. 30-day morbidity, anastomotic leak, re-operation, length of stay and readmission rates were equal between the 2D and 3D arms.
Conclusion: Feasibility of performing multicentre 3D laparoscopic multicentre trials of specialist performed complex procedures is shown. 3D imaging did not alter the number of intraoperative adverse events; however, a potential improvement in mesorectal specimen quality was observed and should form the focus of future 3D laparoscopic TME trials.
Keywords: 3D; Laparoscopic; Rectal cancer; Three-dimensional; Total mesorectal excision; Trial.
Conflict of interest statement
N. J. Curtis, J. A. Conti, R. Dalton, T. A. Rockall, A. S. Allison, J. B. Ockrim, I. C. Jourdan, J. Torkington, S. Phillips, J. Allison, G. B. Hanna, and N. K. Francis confirm they hold no conflict of interest or financial ties to disclose.
Figures

References
-
- Nagtegaal ID, van de Velde CJ, van der Worp E, Kapiteijn E, Quirke P, van Krieken JH. Macroscopic evaluation of rectal cancer resection specimen: clinical significance of the pathologist in quality control. J Clin Oncol. 2002;20(7):1729–1734. - PubMed
-
- Quirke P, Steele R, Monson J, Grieve R, Khanna S, Couture J, et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet. 2009;373(9666):821–828. - PMC - PubMed
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1(8496):1479–1482. - PubMed
-
- Leonard D, Penninckx F, Laenen A, Kartheuser A. Scoring the quality of total mesorectal excision for the prediction of cancer-specific outcome. Colorectal Dis. 2015;17(5):O115–O122. - PubMed
