

Positive end-expiratory pressure titration with electrical impedance tomography and pressure-volume curve in severe acute respiratory distress syndrome
- PMID: 30656479
- PMCID: PMC6336593
- DOI: 10.1186/s13613-019-0484-0
Positive end-expiratory pressure titration with electrical impedance tomography and pressure-volume curve in severe acute respiratory distress syndrome
Abstract
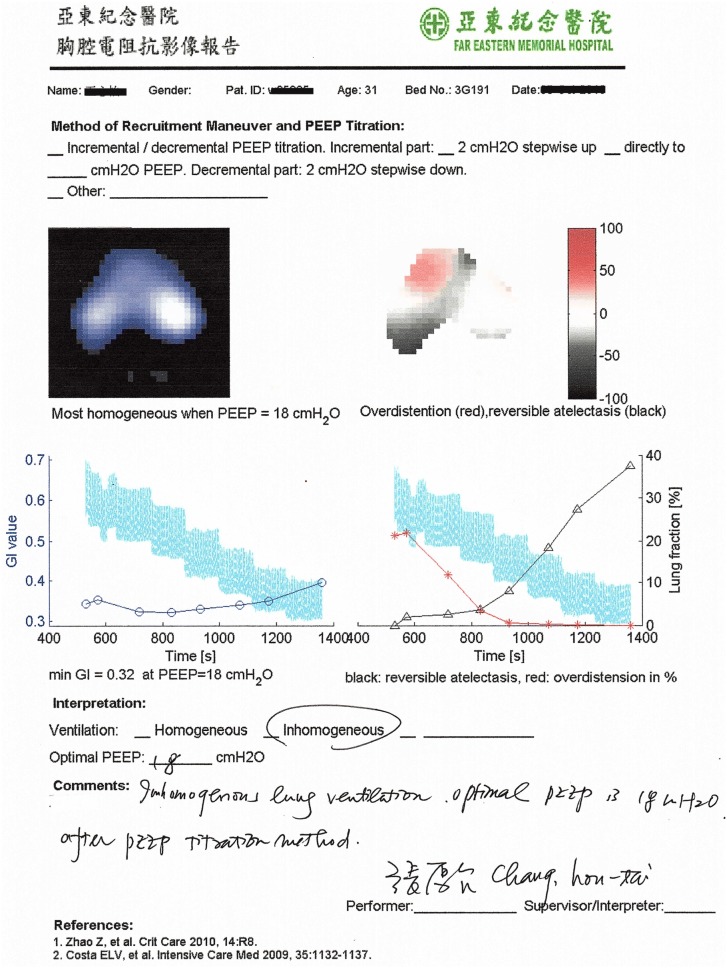
Background: The study objective was to compare titration of positive end-expiratory pressure (PEEP) with electrical impedance tomography (EIT) and with ventilator-embedded pressure-volume loop in severe acute respiratory distress syndrome (ARDS).
Methods: We have designed a prospective study with historical control group. Twenty-four severe ARDS patients (arterial oxygen partial pressure to fractional inspired oxygen ratio, PaO2/FiO2 < 100 mmHg) were included in the EIT group and examined prospectively. Data from another 31 severe ARDS patients were evaluated retrospectively (control group). All patients were receiving medical care under identical general support guidelines and protective mechanical ventilation. The PEEP level selected in the EIT group was the intercept point of cumulated collapse and overdistension percentages curves. In the control group, optimal PEEP was selected 2 cmH2O above the lower inflection point on the static pressure-volume curve.
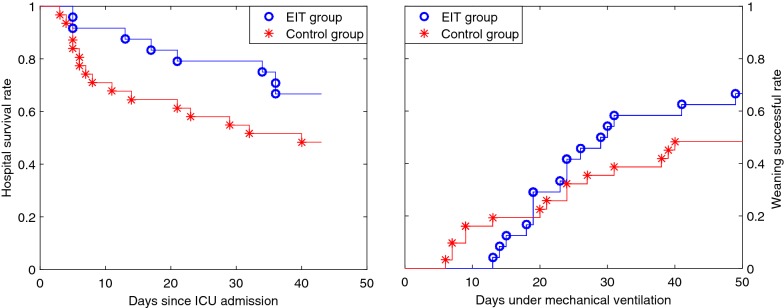
Results: Patients in the EIT group were younger (P < 0.05), and their mean plateau pressure was 1.5 cmH2O higher (P < 0.01). No differences in other baseline parameters such as APACHE II score, PaO2/FiO2, initial PEEP, driving pressure, tidal volume, and respiratory system compliance were found. Two hours after the first PEEP titration, significantly higher PEEP, compliance, and lower driving pressure were found in the EIT group (P < 0.01). Hospital survival rates were 66.7% (16 of 24 patients) in the EIT group and 48.4% (15 of 31) in the control group. Identical rates were found regarding the weaning success rate: 66.7% in the EIT group and 48.4% in the control group.
Conclusion: In severe ARDS patients, it was feasible and safe to guide PEEP titration with EIT at the bedside. As compared with pressure-volume curve, the EIT-guided PEEP titration may be associated with improved oxygenation, compliance, driving pressure, and weaning success rate. The findings encourage further randomized control study with a larger sample size and potentially less bias in the baseline data. Trial Registration NCT03112512.
Keywords: Acute respiratory distress syndrome; Electrical impedance tomography; Lung protective ventilation strategy; Pressure–volume curve; Titration of positive end-expiratory pressure.
Figures
References
-
- Ferguson ND, Fan E, Camporota L, Antonelli M, Anzueto A, Beale R, Brochard L, Brower R, Esteban A, Gattinoni L, et al. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med. 2012;38(10):1573–1582. doi: 10.1007/s00134-012-2682-1. - DOI - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, Davies AR, Hand LE, Zhou Q, Thabane L, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299(6):637–645. doi: 10.1001/jama.299.6.637. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
