

Association of Adverse Effects of Medical Treatment With Mortality in the United States: A Secondary Analysis of the Global Burden of Diseases, Injuries, and Risk Factors Study
- PMID: 30657530
- PMCID: PMC6484545
- DOI: 10.1001/jamanetworkopen.2018.7041
Association of Adverse Effects of Medical Treatment With Mortality in the United States: A Secondary Analysis of the Global Burden of Diseases, Injuries, and Risk Factors Study
Abstract
Importance: More than 20 years have passed since the first publication of estimates of the extent of medical harm occurring in hospitals in the United States. Since then, considerable resources have been allocated to improve patient safety, yet policymakers lack a clear gauge of the progress made.
Objectives: To quantify the cause-specific mortality associated with adverse effects of medical treatment (AEMT) in the United States from 1990 to 2016 by age group, sex, and state of residence and to describe trends in types of harm and associations with other diseases and injuries.
Design, setting, and participants: Cohort study using 1990-2016 data on mortality due to AEMT from the Global Burden of Diseases, Injuries, and Risk Factors (GBD) 2016 study, which assessed death certificates of US decedents.
Exposures: Death with International Classification of Diseases (ICD)-coded registration.
Main outcomes and measures: Mortality associated with AEMT. Secondary analyses were performed on all ICD codes in the death certificate's causal chain to describe associations between AEMT and other diseases and injuries.
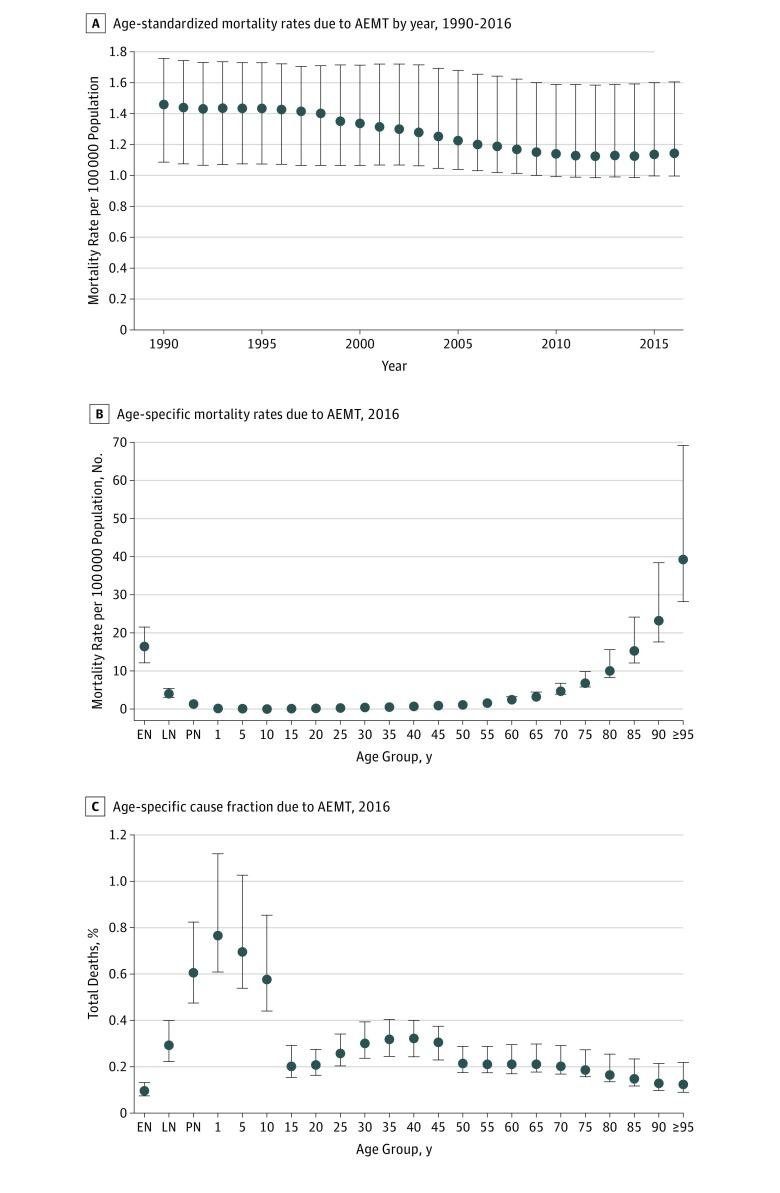
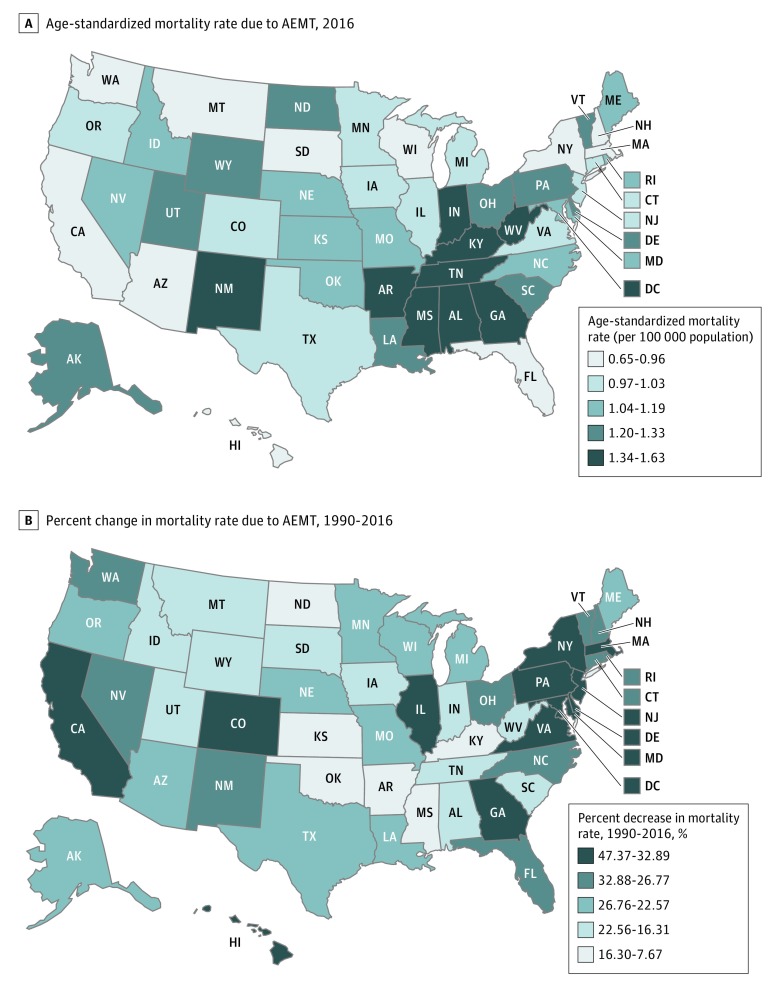
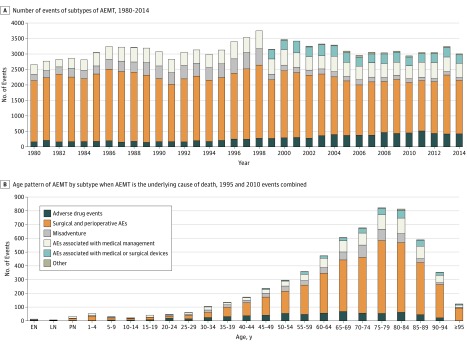
Results: From 1990 to 2016, there were an estimated 123 603 deaths (95% uncertainty interval [UI], 100 856-163 814 deaths) with AEMT as the underlying cause. Despite an overall increase in the number of deaths due to AEMT over time, the national age-standardized mortality rate due to AEMT decreased by 21.4% (95% UI, 1.3%-32.2%) from 1.46 (95% UI, 1.09-1.76) deaths per 100 000 population in 1990 to 1.15 (95% UI, 1.00-1.60) deaths per 100 000 population in 2016. Men and women had similar rates of AEMT mortality, and those 70 years or older had mortality rates nearly 20-fold greater compared with those aged 15 to 49 years (mortality rate in 2016 for both sexes, 7.93 [95% UI, 7.23-11.45] per 100 000 population for those aged ≥70 years vs 0.38 [95% UI, 0.34-0.43] per 100 000 population for those aged 15-49 years). Per 100 000 population, California had the lowest age-standardized AEMT mortality rate at 0.84 deaths (95% UI, 0.57-1.47 deaths), whereas Mississippi had the highest mortality rate at 1.67 deaths (95% UI, 1.19-2.03 deaths). Surgical and perioperative events were the most common subtype of AEMT, accounting for 63.6% of all deaths for which an AEMT was identified as the underlying cause.
Conclusions and relevance: This study's findings suggest a modest reduction in the mortality rate associated with AEMT in the United States from 1990 to 2016 while also observing increased mortality associated with advancing age and noted geographic variability. The annual GBD releases may allow for tracking of the burden of AEMT in the United States.
Conflict of interest statement
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, DC: National Academies Press; 1999. - PubMed
-
- Institute for Health Care Improvement. Protecting 5 million lives from harm. http://www.ihi.org/Engage/Initiatives/Completed/5MillionLivesCampaign/Pa.... Accessed November 18, 2016.
