

"In the United States, we say, 'No breastfeeding,' but that is no longer realistic": provider perspectives towards infant feeding among women living with HIV in the United States
- PMID: 30657639
- PMCID: PMC6338297
- DOI: 10.1002/jia2.25224
"In the United States, we say, 'No breastfeeding,' but that is no longer realistic": provider perspectives towards infant feeding among women living with HIV in the United States
Abstract
Introduction: Currently, the United States (U.S.) recommends that infants born to women living with HIV (WLHIV) be fed formula, whereas many low-resource settings follow the World Health Organization's recommendation to exclusively breastfeed with ongoing antiretroviral therapy. Evidence on infant feeding among WLHIV in high-resource countries suggest that these contrasting recommendations create challenges for providers and patients. Our study used multiple methods to understand providers' infant feeding perspectives on caring for their pregnant and post-partum WLHIV in the U.S.
Methods: We sent a survey (n = 93) to providers across the U.S. who have cared for WLHIV. A subset of survey participants opted into a follow-up qualitative interview (n = 21). These methods allowed us to capture a broad understanding of provider attitudes via the survey and more nuanced qualitative interviews. The study was completed prior to an updated breastfeeding section of the U.S. Perinatal Guidelines.
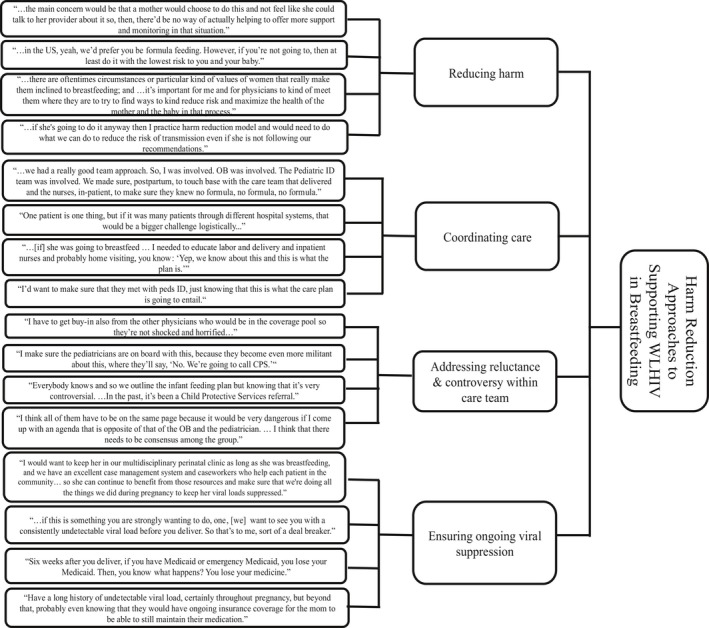
Results: The majority of providers (66.7%) discussed infant feeding intent with their patients using open-ended questions. Many also discussed alternative feeding methods (37.6%) and disclosure avoidance strategies (34.4%). Over 75% (95% confidence interval (CI): 65.1 to 84.2) of participants reported that a WLHIV asked if she could breastfeed her child, and 29% (95% CI 20 to 40.3) reported caring for a patient who breastfed despite recommendations against breastfeeding. Providers reported that their patients' primary concern was stigma associated with not breastfeeding (58%), while providers were primarily concerned about medication adherence during breastfeeding (70%). Through qualitative analysis, four overarching categories emerged that reflect providers' sentiments, including (1) U.S. guidelines inadequately addressing WLHIV's desire to breastfeed; (2) negotiating patient autonomy amidst complex feeding situations; (3) harm reduction approaches to supporting WLHIV in breastfeeding; and (4) providers anticipating multilayered patient stigmatization.
Conclusions: The majority of provider respondents cared for a WLHIV who desired to breastfeed, and a third had WLHIV who breastfed despite recommendations against it. Providers found that the status of U.S. guidelines and their incongruity with WHO guidelines left them without adequate resources to support WLHIV's infant feeding decisions. Our findings provide important insight to inform professional associations' discussions about public health policy as they consider future directions for infant feeding guidelines among WLHIV.
Keywords: HIV; United States; breastfeeding; harm reduction; infant feeding; provider attitudes.
© 2019 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- U.S. Department of Health and Human Services Panel on Treatment of HIV‐Infected Pregnant Women and Prevention of Perinatal Transmission . Recommendations for Use of Antiretroviral Drugs in Pregnant HIV‐1‐Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. 2017. [cited 2018 March 26]. Available from: http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf
-
- U.S. Department of Health and Human Services AIDSinfo . Recommendations for the Use of Antiretroviral Drugs in Pregnant Women with HIV Infection and Interventions to Reduce Perinatal HIV Transmission in the United States. 2018. [Cited 2018 Sept 16]. Available from: https://aidsinfo.nih.gov/guidelines/html/3/perinatal/513/guidance-for-co...
-
- Flynn PM, Taha TE, Cababasay M, Fowler MG, Mofenson LM, Owor M, et al. Prevention of HIV‐1 transmission through breastfeeding: efficacy and safety of maternal antiretroviral therapy versus infant nevirapine prophylaxis for duration of breastfeeding in HIV‐1‐infected women with high CD4 cell count (IMPAACT PROMISE): a randomized, open‐label, clinical trial. J Acuir Immune Defic Syndr. 2018;77(4):383–92. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
