

Tetralogy of Fallot: morphological variations and implications for surgical repair
- PMID: 30657877
- PMCID: PMC6580293
- DOI: 10.1093/ejcts/ezy474
Tetralogy of Fallot: morphological variations and implications for surgical repair
Abstract
Objectives: Tetralogy of Fallot is characterized by anterocephalad deviation of the outlet septum, along with abnormal septoparietal trabeculations, which lead to subpulmonary infundibular stenosis. Archives of retained hearts are an important resource for improving our understanding of congenital heart defects and their morphological variability. This study aims to define variations in aortic override, coronary arterial patterns and ventricular septal defects in tetralogy of Fallot as observed in a morphological archive, highlighting implications for surgical management.
Methods: The Birmingham Children's Hospital archive contains 211 hearts with tetralogy of Fallot, of which 164 were analysed [69 (42.1%) unrepaired and 95 (57.9%) operated specimens]. A detailed morphological and geometric analysis was performed using a rigorous 5-layer review process.
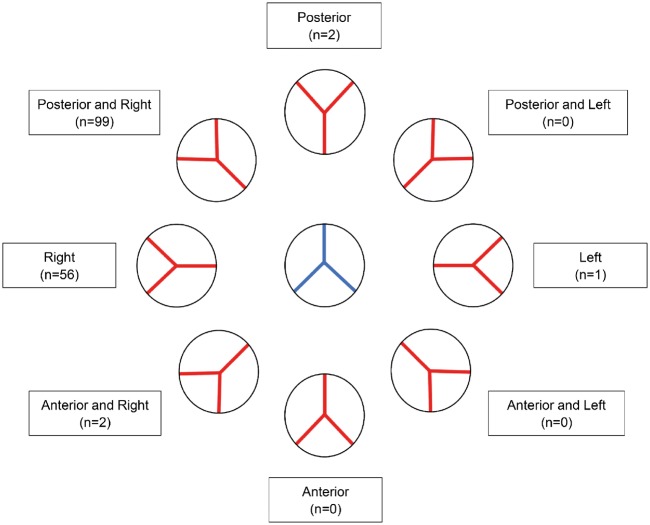
Results: Anomalies were observed in the orifices, origins and course of the coronary arteries: 20 hearts (13.0%) had more than 2 orifices and 3 hearts (1.9%) had a single orifice. In 7 hearts (4.3%), a coronary artery crossed the right ventricular outflow tract. The extent of aortic override ranged from 31.0% to 100% (median of 59.5%). The ventricular septal defect was most often perimembranous (139, 84.8%), but we also found muscular (14, 8.5%), atrioventricular (7, 4.3%) and doubly committed juxta-arterial (2, 1.2%) variants.
Conclusions: Anatomical variations are common and can impact surgical management. Anomalous coronary arteries may require a conduit rather than a transannular patch. Variability in aortic override determines the size of patch used to baffle blood to the aorta. The type of ventricular septal defect affects patch closure and the risk of postoperative conduction defects.
Keywords: Aortic override; Cardiac surgery; Coronary arteries; Morphology; Tetralogy of Fallot.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures







References
-
- Evans WN. “Tetralogy of Fallot” and Étienne-Louis Arthur Fallot. Pediatr Cardiol 2008;29:637–40. - PubMed
-
- Anderson RH, Moorman A, Brown N, Bamforth S, Chaudhry B, Henderson D. et al. Normal and abnormal development of the heart In: Da Cruz E, Ivy D, Jaggers J (eds). Pediatric and Congenital Cardiology, Cardiac Surgery and Intensive Care. London: Springer, 2013, 151–77.
-
- Anderson RH, Webb S, Brown NA.. Establishing the anatomic hallmarks of congenitally malformed hearts. Trends Cardiovasc Med 1996;6:10–15. - PubMed
-
- van Praagh R. The first Stella van Praagh memorial lecture: the history and anatomy of tetralogy of Fallot. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2009;12:19–38. - PubMed
-
- Anderson RH, Tynan M.. Tetralogy of Fallot—a centennial review. Int J Cardiol 1988;21:219–32. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
