

Thyroid Abnormalities in Patients With Extreme Insulin Resistance Syndromes
- PMID: 30657911
- PMCID: PMC6482021
- DOI: 10.1210/jc.2018-02289
Thyroid Abnormalities in Patients With Extreme Insulin Resistance Syndromes
Abstract
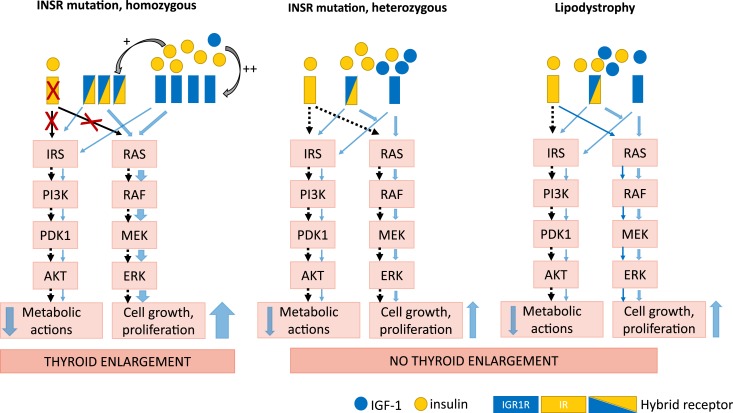
Context: Insulin and leptin may increase growth and proliferation of thyroid cells, underlying an association between type 2 diabetes and papillary thyroid cancer (PTC). Patients with extreme insulin resistance due to lipodystrophy or insulin receptor mutations (INSR) are treated with high-dose insulin and recombinant leptin (metreleptin), which may increase the risk of thyroid neoplasia.
Objective: The aim of this study was to analyze thyroid structural abnormalities in patients with lipodystrophy and INSR mutations and to assess whether insulin, IGF-1, and metreleptin therapy contribute to the thyroid growth and neoplasia in this population.
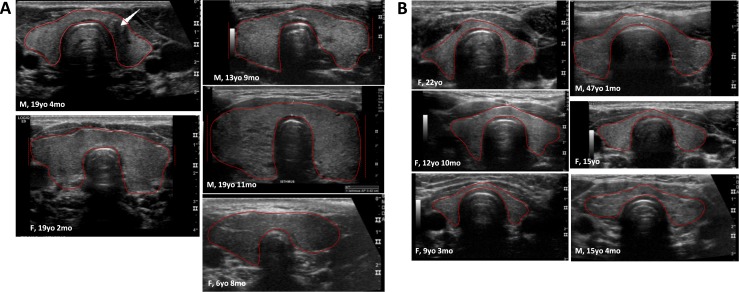
Design: Thyroid ultrasound characteristics were analyzed in 81 patients with lipodystrophy and 11 with INSR (5 homozygous; 6 heterozygous). Sixty patients were taking metreleptin.
Results: The prevalence of thyroid nodules in children with extreme insulin resistance (5 of 30, 16.7%) was significantly higher than published prevalence for children (64 of 3202; 2%), with no difference between lipodystrophy and INSR. Body surface area-adjusted thyroid volume was larger in INSR homozygotes vs heterozygotes or lipodystrophy (10.4 ± 5.1, 3.9 ± 1.5, and 6.2 ± 3.4 cm2, respectively. Three patients with lipodystrophy and one INSR heterozygote had PTC. There were no differences in thyroid ultrasound features in patients treated vs not treated with metreleptin.
Conclusion: Children with extreme insulin resistance had a high prevalence of thyroid nodules, which were not associated with metreleptin treatment. Patients with homozygous INSR mutation had thyromegaly, which may be a novel phenotypic feature of this disease. Further studies are needed to determine the etiology of thyroid abnormalities in patients with extreme insulin resistance.
Published by Oxford University Press on behalf of the Endocrine Society 2019.
Figures
References
-
- Lee MY, Lin KD, Hsiao PJ, Shin SJ. The association of diabetes mellitus with liver, colon, lung, and prostate cancer is independent of hypertension, hyperlipidemia, and gout in Taiwanese patients. Metabolism. 2012;61(2):242–249. - PubMed
-
- Tanaka K, Tsuji I, Tamakoshi A, Matsuo K, Wakai K, Nagata C, Mizoue T, Inoue M, Tsugane S, Sasazuki S; Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan . Diabetes mellitus and liver cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn J Clin Oncol. 2014;44(10):986–999. - PubMed
-
- Weiderpass E, Gridley G, Persson I, Nyrén O, Ekbom A, Adami HO. Risk of endometrial and breast cancer in patients with diabetes mellitus. Int J Cancer. 1997;71(3):360–363. - PubMed
-
- Noto H, Tsujimoto T, Sasazuki T, Noda M. Significantly increased risk of cancer in patients with diabetes mellitus: a systematic review and meta-analysis. Endocr Pract. 2011;17(4):616–628. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
