

Constipation and risk of death and cardiovascular events
- PMID: 30658186
- PMCID: PMC6399019
- DOI: 10.1016/j.atherosclerosis.2018.12.021
Constipation and risk of death and cardiovascular events
Abstract
Background and aims: Constipation is one of the most frequent symptoms encountered in daily clinical practice and is implicated in the development of atherosclerosis, potentially through altered gut microbiota. However, little is known about its association with incident cardiovascular events.
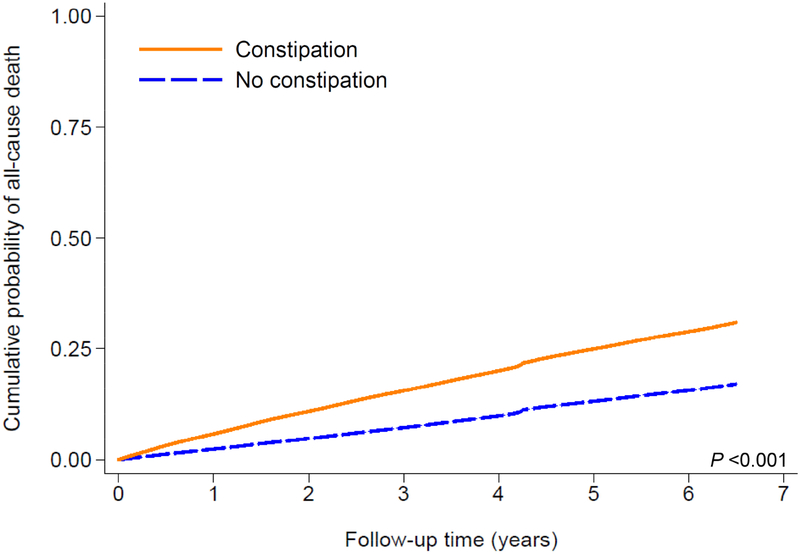
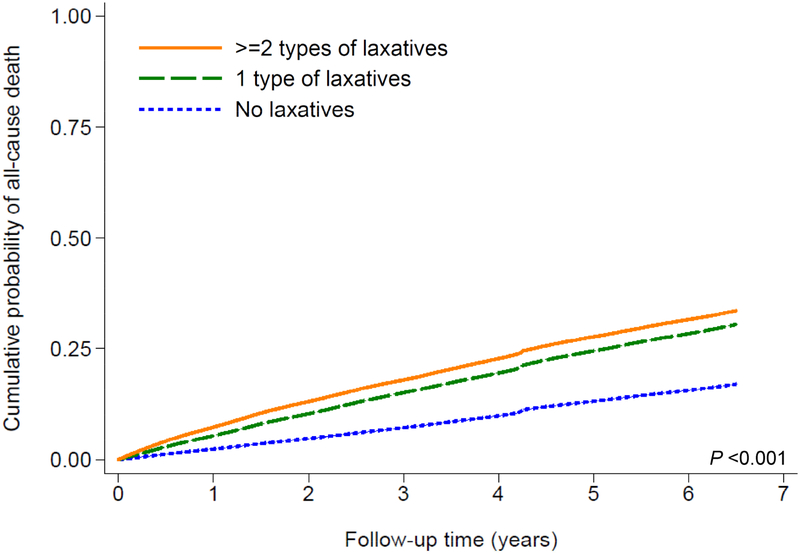
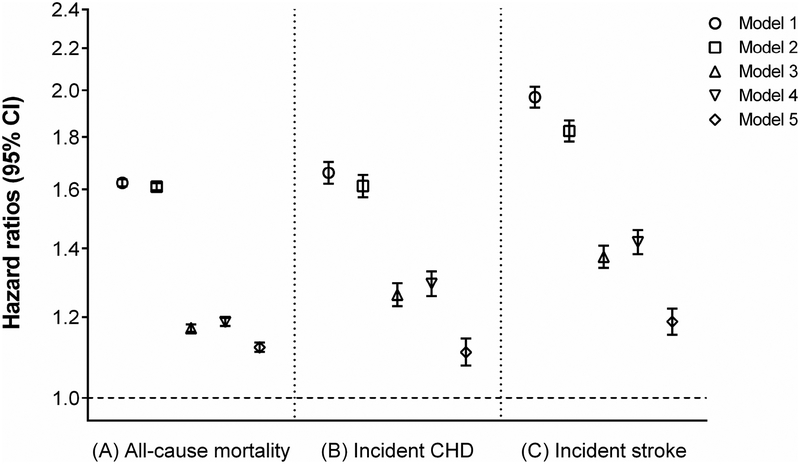
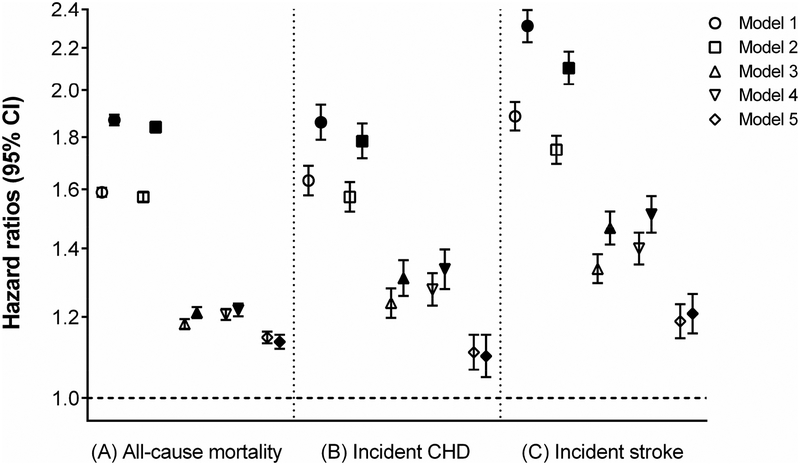
Methods: In a nationally representative cohort of 3,359,653 US veterans with an estimated glomerular filtration rate (eGFR) ≥60 mL/min/1.73 m2 between October 1, 2004 and September 30, 2006 (baseline period), with follow-up through 2013, we examined the association of constipation status (absence or presence; defined using diagnostic codes and laxative use) and laxative use (none, one, or ≥2 types of laxatives) with all-cause mortality, incident coronary heart disease (CHD), and incident ischemic stroke.
Results: Among 3,359,653 patients, 237,855 (7.1%) were identified as having constipation. After multivariable adjustments for demographics, prevalent comorbidities, medications, and socioeconomic status, patients with (versus without) constipation had 12% higher all-cause mortality (hazard ratio [HR], 1.12; 95% CI, 1.11-1.13), 11% higher incidence of CHD (HR, 1.11; 95% CI, 1.08-1.14), and 19% higher incidence of ischemic stroke (HR, 1.19; 95% CI, 1.15-1.22). Patients with one and ≥2 (versus none) types of laxatives experienced a similarly higher risk of all-cause mortality (HRs [95% CI], 1.15 [1.13-1.16] and 1.14 [1.12-1.15], respectively), incident CHD (HRs [95% CI], 1.11 [1.07-1.15] and 1.10 [1.05-1.15], respectively) and incident ischemic stroke (HRs [95% CI], 1.19 [1.14-1.23] and 1.21 [1.16-1.26], respectively).
Conclusions: Constipation status and laxative use are independently associated with higher risk of all-cause mortality and incident CHD and ischemic stroke.
Keywords: Constipation; Coronary heart disease; Laxatives; Mortality; Stroke.
Published by Elsevier B.V.
Conflict of interest statement
Conflict of interest:
Drs. Kovesdy and Kalantar-Zadeh are employees of the US Department of Veterans affairs. Opinions expressed in this paper are those of the authors’ and do not necessarily represent the opinion of the Department of Veterans Affairs. All authors had access to the data and a role in writing the manuscript.
None of the authors have relevant conflicts of interest.
Figures
References
-
- Dennison C, Prasad M, Lloyd A, Bhattacharyya SK, Dhawan R, Coyne K. The health-related quality of life and economic burden of constipation. Pharmacoeconomics 2005;23(5):461–476. - PubMed
-
- Sun SX, Dibonaventura M, Purayidathil FW, Wagner JS, Dabbous O, Mody R. Impact of chronic constipation on health-related quality of life, work productivity, and healthcare resource use: an analysis of the National Health and Wellness Survey. Dig. Dis. Sci 2011;56(9):2688–2695. - PubMed
-
- Guerin A, Carson RT, Lewis B, Yin D, Kaminsky M, Wu E. The economic burden of treatment failure amongst patients with irritable bowel syndrome with constipation or chronic constipation: a retrospective analysis of a Medicaid population. J. Med. Econ 2014;17(8): 577–586. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
