

Evaluating Hospital Readmissions for Persons With Serious and Complex Illness: A Competing Risks Approach
- PMID: 30658539
- PMCID: PMC9451045
- DOI: 10.1177/1077558718823919
Evaluating Hospital Readmissions for Persons With Serious and Complex Illness: A Competing Risks Approach
Abstract
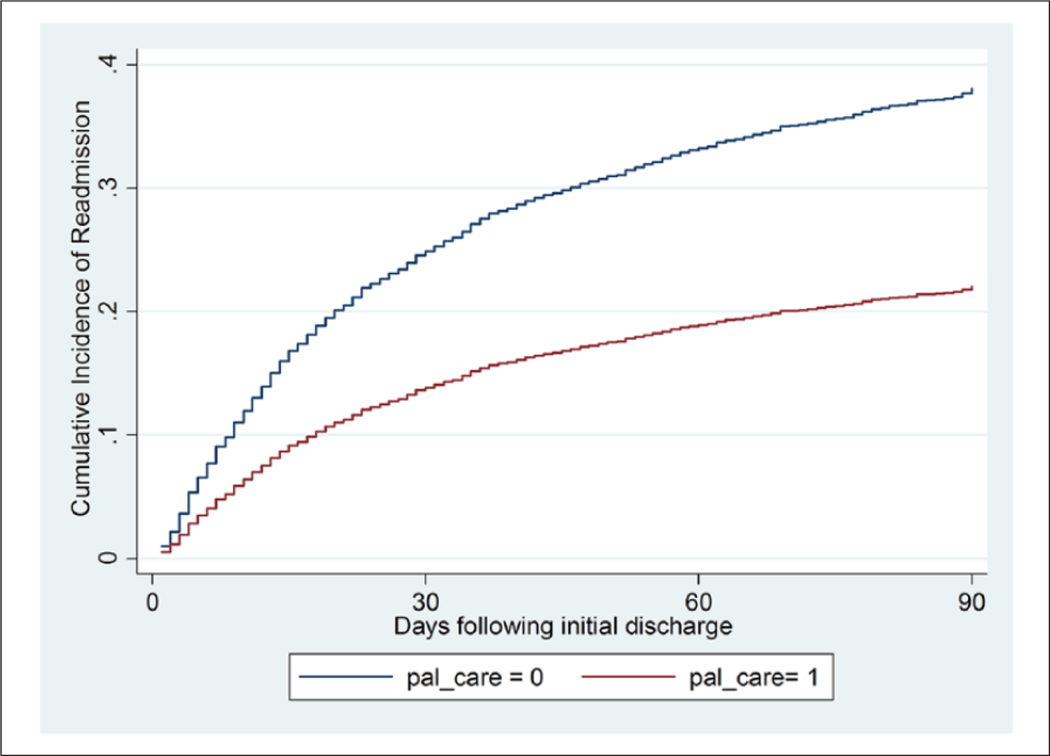
Hospital readmission rate is a ubiquitous measure of efficiency and quality. Individuals with life-limiting illnesses account heavily for admissions but evaluation is complicated by high-mortality rates. We report a retrospective cohort study examining the association between palliative care (PC) and readmissions while controlling for postdischarge mortality with a competing risks approach. Eligible participants were adult inpatients admitted to an academic, safety-net medical center (2009-2015) with at least one diagnosis of cancer, heart failure, chronic obstructive pulmonary disease, liver failure, kidney failure, AIDS/HIV, and selected neurodegenerative conditions. PC was associated with reduced 30-, 60-, and 90-day readmissions (subhazard ratios = 0.57, 0.53, and 0.52, respectively [all p < .001]). Hospital PC is associated with a reduction in readmissions, and this is not explained by higher mortality among PC patients. Performance measures only counting those alive at a given end point may underestimate systematically the effects of treatments with a high-mortality rate.
Keywords: hospital readmissions; mortality; palliative care; retrospective studies.
Figures
Similar articles
-
Association of short-term exposure to ambient PM2.5 with hospital admissions and 30-day readmissions in end-stage renal disease patients: population-based retrospective cohort study.BMJ Open. 2020 Dec 15;10(12):e041177. doi: 10.1136/bmjopen-2020-041177. BMJ Open. 2020. PMID: 33323443 Free PMC article.
-
Comparison of Mortality and Hospital Readmissions Among Patients Receiving Virtual Ward Transitional Care vs Usual Postdischarge Care: A Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Jun 1;5(6):e2219113. doi: 10.1001/jamanetworkopen.2022.19113. JAMA Netw Open. 2022. PMID: 35763296 Free PMC article.
-
Readmissions Reduction Program: Mortality and Readmissions for Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2021 Feb 15;203(4):437-446. doi: 10.1164/rccm.202002-0310OC. Am J Respir Crit Care Med. 2021. PMID: 32871097 Free PMC article.
-
The association of acute kidney injury in the critically ill and postdischarge outcomes: a cohort study*.Crit Care Med. 2015 Feb;43(2):354-64. doi: 10.1097/CCM.0000000000000706. Crit Care Med. 2015. PMID: 25474534
-
Association between interhospital care fragmentation, readmission diagnosis, and outcomes.Am J Manag Care. 2021 May 1;27(5):e164-e170. doi: 10.37765/ajmc.2021.88639. Am J Manag Care. 2021. PMID: 34002968
Cited by
-
Using predicted length of stay to define treatment and model costs in hospitalized adults with serious illness: an evaluation of palliative care.Health Econ Rev. 2021 Sep 20;11(1):38. doi: 10.1186/s13561-021-00336-w. Health Econ Rev. 2021. PMID: 34542719 Free PMC article.
-
Local Supply Of Postdischarge Care Options Tied To Hospital Readmission Rates.Health Aff (Millwood). 2022 Jul;41(7):1036-1044. doi: 10.1377/hlthaff.2021.01991. Health Aff (Millwood). 2022. PMID: 35787076 Free PMC article.
-
Economic Analysis of Hospital Palliative Care: Investigating Heterogeneity by Noncancer Diagnoses.MDM Policy Pract. 2019 Sep 10;4(2):2381468319866451. doi: 10.1177/2381468319866451. eCollection 2019 Jul-Dec. MDM Policy Pract. 2019. PMID: 31535032 Free PMC article.
-
Increased Retention in Care After a Palliative Care Referral Among People Living With HIV.J Acquir Immune Defic Syndr. 2020 May 1;84(1):78-84. doi: 10.1097/QAI.0000000000002296. J Acquir Immune Defic Syndr. 2020. PMID: 31923086 Free PMC article.
-
Cost consequences of unscheduled emergency admissions in cancer patients in the last year of life.Support Care Cancer. 2023 Mar 4;31(3):201. doi: 10.1007/s00520-023-07633-6. Support Care Cancer. 2023. PMID: 36869930 Free PMC article.
References
-
- Bakitas M, Tosteson T, Li Z, Lyons K, Hull J, Li Z, . . . Dragnev KH (2014). The ENABLE III randomized controlled trial of concurrent palliative oncology care. Paper presented at the ASCO Annual Meeting, Chicago, IL.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
