

Does movement matter in people with back pain? Investigating 'atypical' lumbo-pelvic kinematics in people with and without back pain using wireless movement sensors
- PMID: 30658610
- PMCID: PMC6339318
- DOI: 10.1186/s12891-018-2387-x
Does movement matter in people with back pain? Investigating 'atypical' lumbo-pelvic kinematics in people with and without back pain using wireless movement sensors
Abstract
Background: Interventions for low back pain (LBP) commonly target 'dysfunctional' or atypical lumbo-pelvic kinematics in the belief that correcting aberrant movement improves patients' pain and activity outcomes. If atypical kinematic parameters and postures have a relationship to LBP, they could be expected to more prevalent in people with LBP compared to people without LBP (NoLBP). This exploratory study measured, defined and compared atypical kinematic parameters in people with and without LBP.
Methods: Wireless inertial motion and EMG sensors were used to measure lumbo-pelvic kinematics during standing trunk flexion (range of motion (ROM), timing, sequence coordination, and extensor muscle activation) and in sitting (relative sitting position, pelvic tilt range) in a sample of 126 of adults without LBP and 140 chronic LBP subjects. Atypical movement was defined using the 10th/90th centiles of the NoLBP group. Mean differences and prevalence rates for atypical movement were calculated. Dichotomised pain scores for 'high-pain-on-bending' and 'high-pain-on-sitting' were tested for their association with atypical kinematic variables.
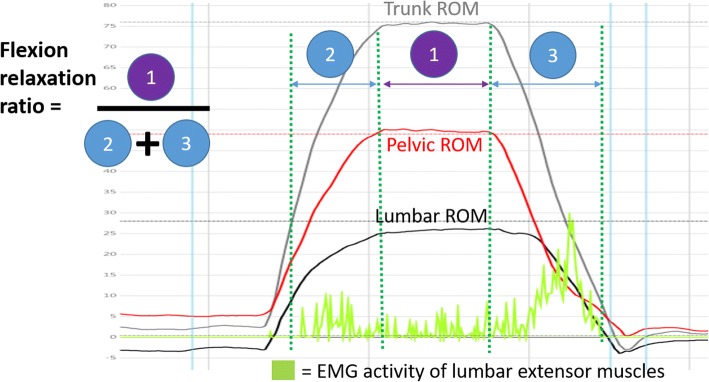
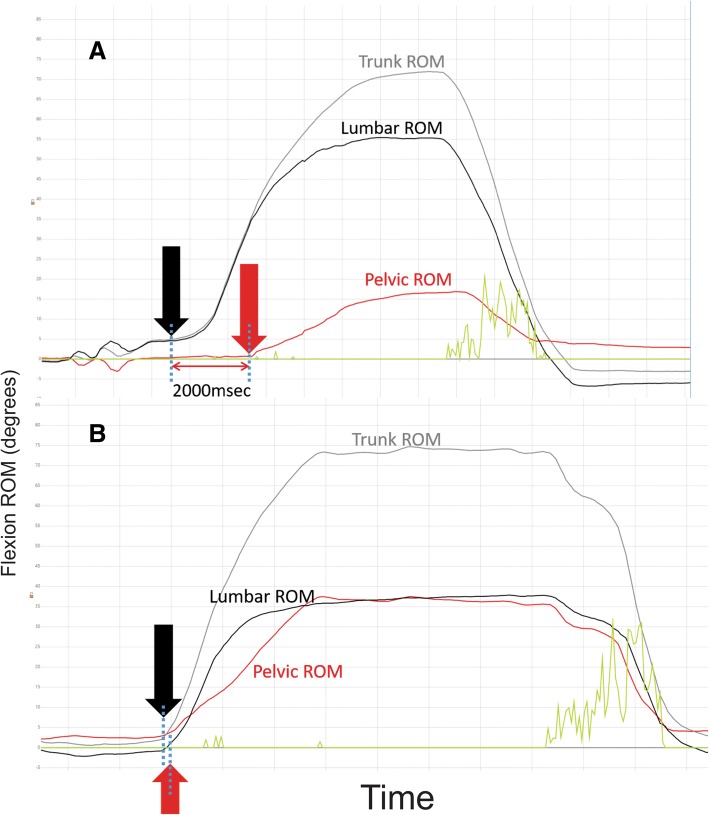
Results: For standing flexion, significant mean differences, after adjusting for age and gender factors, were seen for the LBP group with (i) reduced ROM (trunk flexion (NoLBP 111o, LBP 93o, p < .0001), lumbar flexion (NoLBP 52o, LBP 46o, p < .0001), pelvic flexion (NoLBP 59o, LBP 48o, p < .0001), (ii) greater extensor muscle activation for the LBP group (NoLBP 0.012, LBP 0.25 p < .0001), (iii) a greater delay in pelvic motion at the onset of flexion (NoLBP - 0.21 s; LBP - 0.36 s, p = 0.023), (iv) and longer movement duration for the LBP group (NoLBP 2.28 s; LBP 3.18 s, p < .0001). Atypical movement was significantly more prevalent in the LBP group for small trunk (× 5.4), lumbar (× 3.0) and pelvic ROM (× 3.9), low FRR (× 4.9), delayed pelvic motion at 20o flexion (× 2.9), and longer movement duration (× 4.7). No differences between groups were seen for any sitting parameters. High pain intensity was significantly associated with small lumbar ROM and pelvic ROM.
Conclusion: Significant movement differences during flexion were seen in people with LBP, with a higher prevalence of small ROM, slower movement, delayed pelvic movement and greater lumbar extensor muscle activation but without differences for any sitting parameter.
Keywords: Assessment; Flexion relaxation; Low back pain; Lumbo-pelvic rhythm; Movement disorders; Range of movement (ROM); Velocity.
Conflict of interest statement
Ethics approval and consent to participate
This research project was performed in accordance with the declaration of Helsinki with approval obtained from Monash University Human Research Ethics Committee (approval number CF12/1995–2,012,001,090, 2016–1100) and The Regional Committees on Health Research Ethics for Southern Denmark (approval number S-20110071). All participants gave written informed consent for testing and use of de-identified data, through the use of an ethics committee approved patient information and consent form.
Consent for publication
All participants were provided with a Monash University Human Research Ethics Committee approved patient information and consent form, which included consent for publication. All participants provided signed consent forms before being admitted into the study.
Competing interests
No benefits in any form have been, or will be, received for this study from a commercial party related directly or indirectly to the subject of this paper. This paper does not contain information about drugs. The authors do not hold stocks or shares in any company that might be directly or indirectly affected by this study. No patents have been applied for or received due to the content of this paper and there are no non-financial competing interests associated with this paper. The lead author (RL) has been engaged as a consultant by DorsaVi for training clinicians in how to use the ViMove device but otherwise has no financial interest in the company, DorsaVi, nor has received any funding for this study. DorsaVi has a 25% ownership in a private physiotherapy clinic that RL is a director of. PK has received a market-rate consulting fee from DorsaVi for clinical trial design advice unrelated to the current study but otherwise has no financial interest in the company, DorsaVi.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Subgroups of lumbo-pelvic flexion kinematics are present in people with and without persistent low back pain.BMC Musculoskelet Disord. 2018 Aug 28;19(1):309. doi: 10.1186/s12891-018-2233-1. BMC Musculoskelet Disord. 2018. PMID: 30153815 Free PMC article.
-
How consistent are lordosis, range of movement and lumbo-pelvic rhythm in people with and without back pain?BMC Musculoskelet Disord. 2016 Sep 22;17(1):403. doi: 10.1186/s12891-016-1250-1. BMC Musculoskelet Disord. 2016. PMID: 27658946 Free PMC article.
-
Effects of pelvic asymmetry and low back pain on trunk kinematics during sitting: a comparison with standing.Spine (Phila Pa 1976). 2006 Mar 1;31(5):E135-43. doi: 10.1097/01.brs.0000201325.89493.5f. Spine (Phila Pa 1976). 2006. PMID: 16508537
-
Kinematic Characteristics of Sit-to-Stand Movements in Patients With Low Back Pain: A Systematic Review.J Manipulative Physiol Ther. 2019 Sep;42(7):532-540. doi: 10.1016/j.jmpt.2018.12.004. J Manipulative Physiol Ther. 2019. PMID: 31864436
-
Quantifying the lumbar spine movements of surgeons during surgical lists in a teaching hospital.ANZ J Surg. 2019 Mar;89(3):153-158. doi: 10.1111/ans.14812. Epub 2018 Sep 17. ANZ J Surg. 2019. PMID: 30226000 Review.
Cited by
-
One-shoulder carrying school backpack strongly affects gait swing phase and pelvic tilt: a case study.Acta Biomed. 2020 Apr 10;91(3-S):168-170. doi: 10.23750/abm.v91i3-S.9435. Acta Biomed. 2020. PMID: 32275285 Free PMC article.
-
Assessment of Spinal and Pelvic Kinematics Using Inertial Measurement Units in Clinical Subgroups of Persistent Non-Specific Low Back Pain.Sensors (Basel). 2024 Mar 26;24(7):2127. doi: 10.3390/s24072127. Sensors (Basel). 2024. PMID: 38610338 Free PMC article.
-
Measurement properties of 72 movement biomarkers aiming to discriminate non‑specific chronic low back pain patients from an asymptomatic population.Sci Rep. 2023 Apr 20;13(1):6483. doi: 10.1038/s41598-023-33504-5. Sci Rep. 2023. PMID: 37081110 Free PMC article.
-
Subgrouping People With Acute Low Back Pain Based on Psychological, Sensory, and Motor Characteristics: A Cross-Sectional Study.Eur J Pain. 2025 Apr;29(4):e70006. doi: 10.1002/ejp.70006. Eur J Pain. 2025. PMID: 40035340 Free PMC article.
-
Reliability of isometric and isokinetic trunk flexor strength using a functional electromechanical dynamometer.PeerJ. 2019 Oct 18;7:e7883. doi: 10.7717/peerj.7883. eCollection 2019. PeerJ. 2019. PMID: 31695965 Free PMC article.
References
-
- Kent P, Laird R, Haines T. The effect of changing movement and posture using motion-sensor biofeedback, versus guidelines-based care, on the clinical outcomes of people with sub-acute or chronic low back pain-a multicentre, cluster-randomised, placebo-controlled, pilot trial. BMC Musculoskelet Disord. 2015;16:131–150. doi: 10.1186/s12891-015-0591-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
