

Follow-up score, change score or percentage change score for determining clinical important outcome following surgery? An observational study from the Norwegian registry for Spine surgery evaluating patient reported outcome measures in lumbar spinal stenosis and lumbar degenerative spondylolisthesis
- PMID: 30658613
- PMCID: PMC6339296
- DOI: 10.1186/s12891-018-2386-y
Follow-up score, change score or percentage change score for determining clinical important outcome following surgery? An observational study from the Norwegian registry for Spine surgery evaluating patient reported outcome measures in lumbar spinal stenosis and lumbar degenerative spondylolisthesis
Abstract
Background: Assessment of outcomes for spinal surgeries is challenging, and an ideal measurement that reflects all aspects of importance for the patients does not exist. Oswestry Disability Index (ODI), EuroQol (EQ-5D) and Numeric Rating Scales (NRS) for leg pain and for back pain are commonly used patients reported outcome measurements (PROMs). Reporting the proportion of individuals with an outcome of clinical importance is recommended. Knowledge of the ability of PROMs to identify clearly improved patients is essential. The purpose of this study was to search cut-off criteria for PROMs that best reflect an improvement considered by the patients to be of clinical importance.
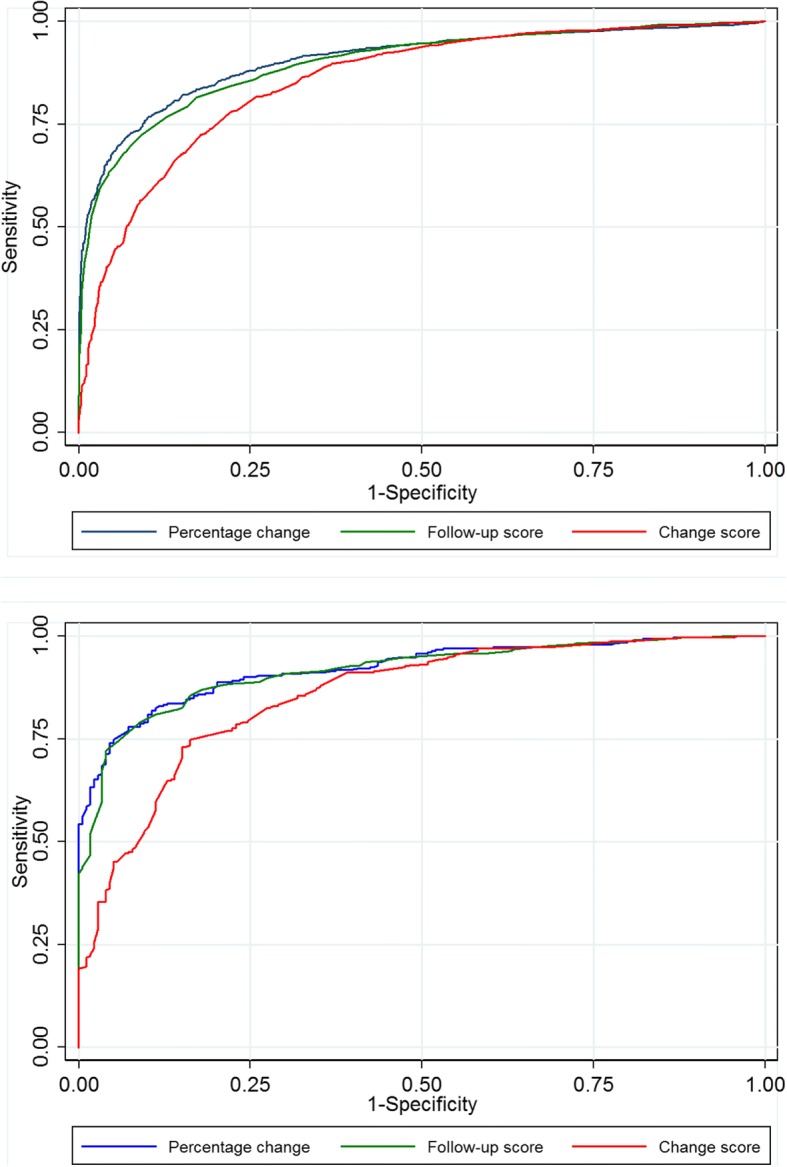
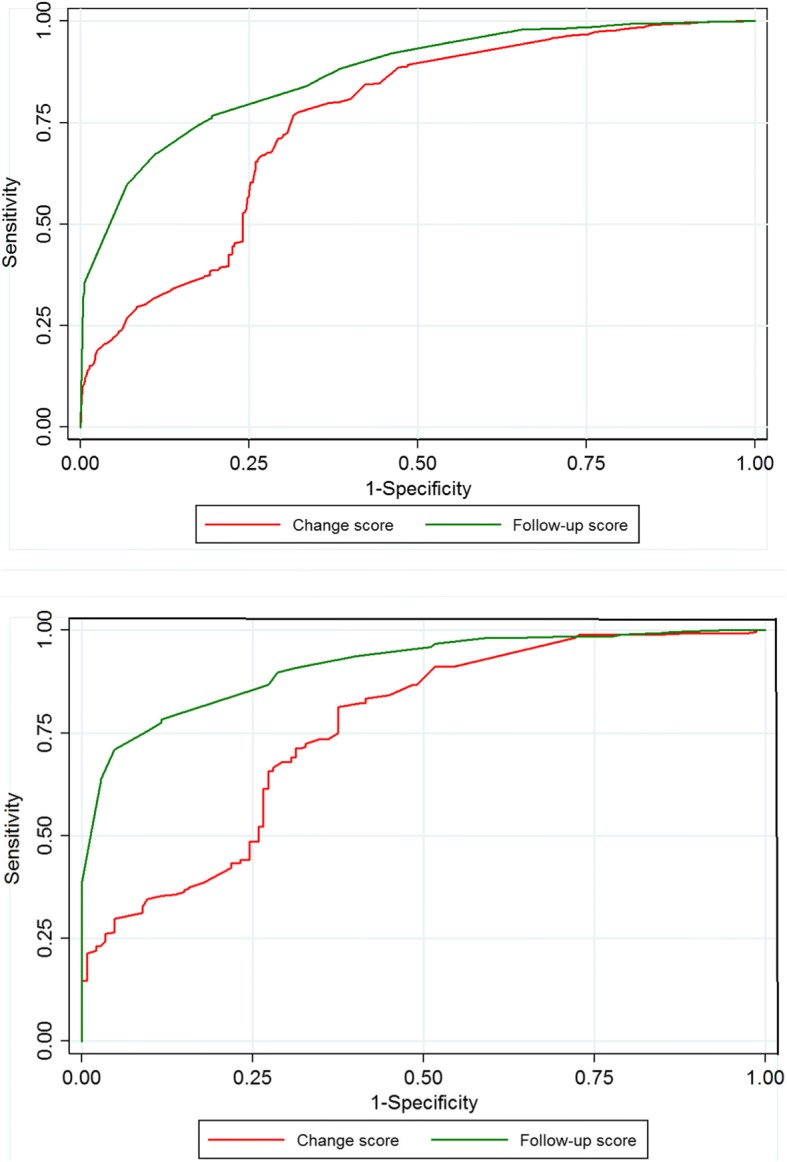
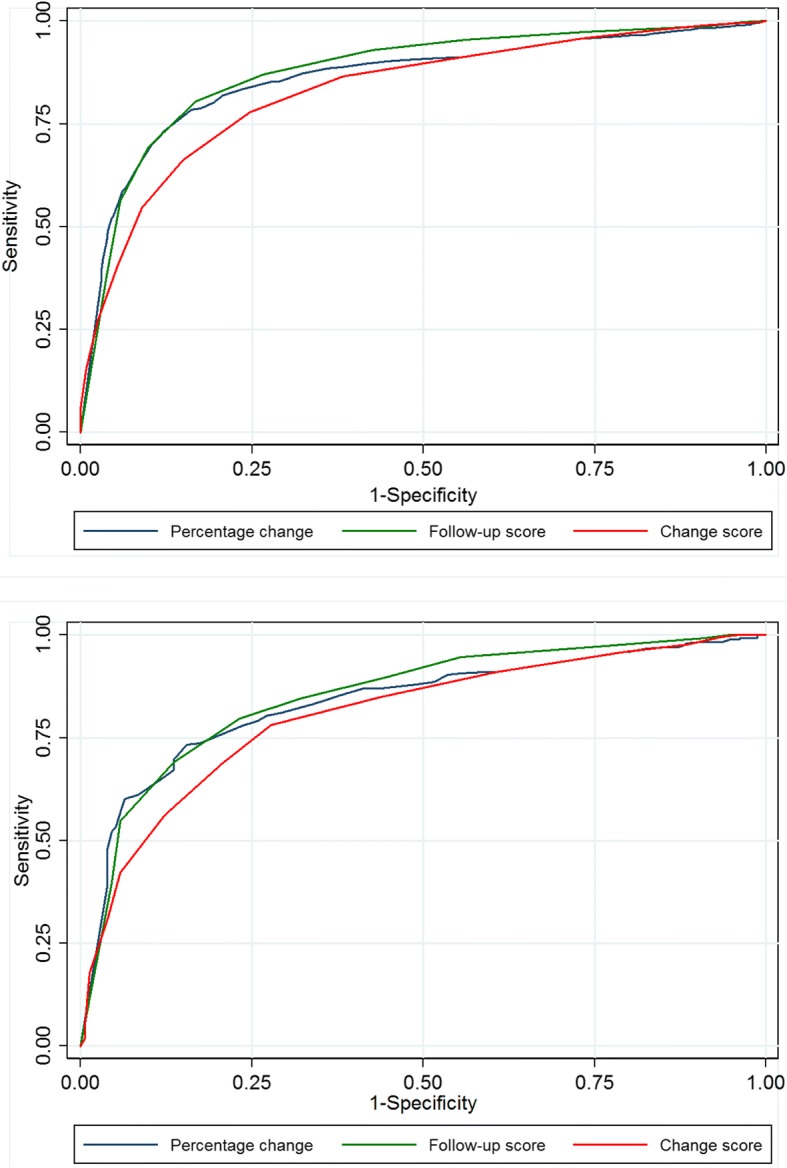
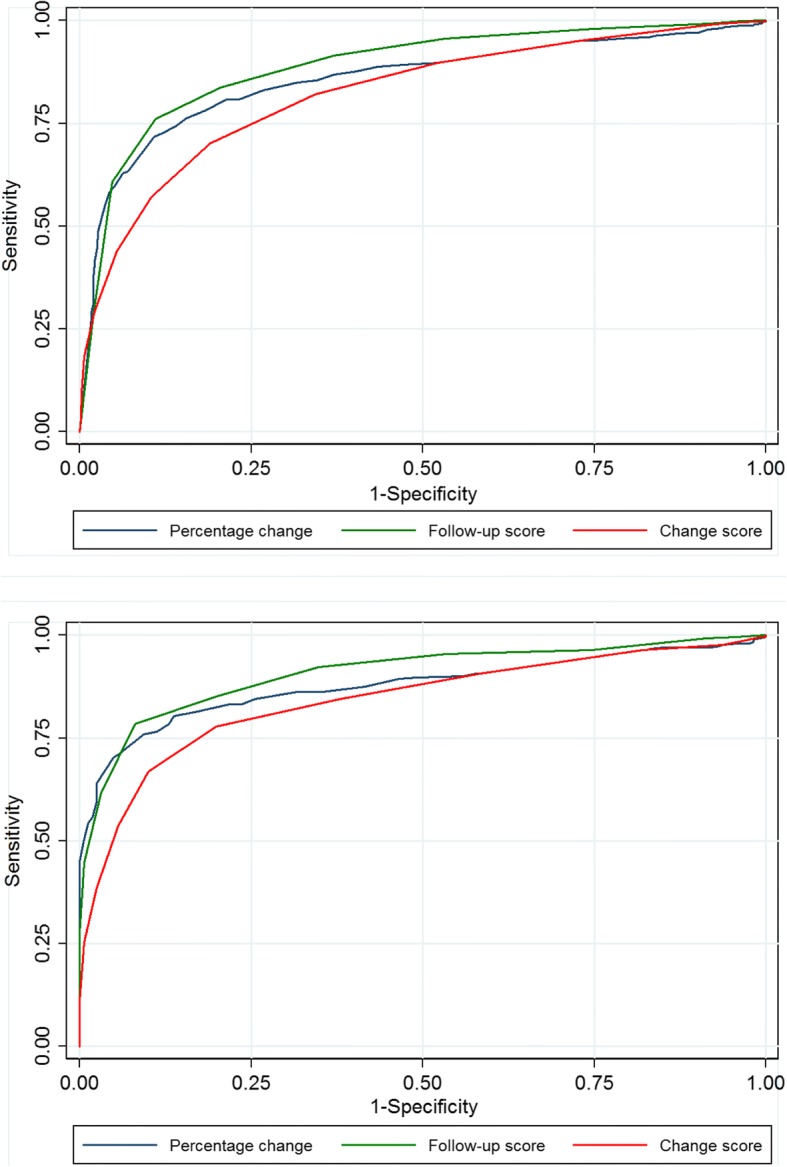
Methods: The Global Perceived Effect scale was utilized to evaluate a clinically important outcome 12 months after surgery. The cut-offs for the PROMs that most accurately distinguish those who reported 'completely recovered' or 'much improved' from those who reported 'slightly improved', unchanged', 'slightly worse', 'much worse', or 'worse than ever' were estimated. For each PROM, we evaluated three candidate response parameters: the (raw) follow-up score, the (numerical) change score, and the percentage change score.
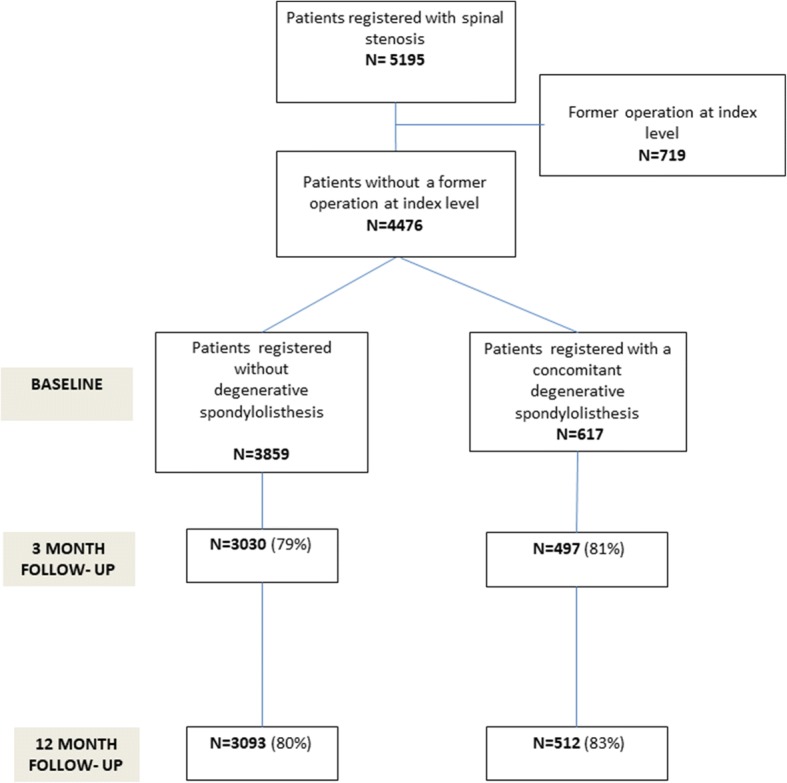
Results: We analysed 3859 patients with Lumbar Spinal Stenosis [(LSS); mean age 66; female gender 50%] and 617 patients with Lumbar Degenerative Spondylolisthesis [(LDS); mean age 67; 72% female gender]. The accuracy of identifying 'completely recovered' and 'much better' patients was generally high, but lower for EQ-5D than for the other PROMs. For all PROMs the accuracy was lower for the change score than for the follow-up score and the percentage change score, especially among patients with low and high PROM scores at baseline. The optimal threshold for a clinically important outcome was ≤24 for ODI, ≥0.69 for EQ-5D, ≤3 for NRS leg pain, and ≤ 4 for NRS back pain, and, for the percentage change score, ≥30% for ODI, ≥40% for NRS leg pain, and ≥ 33% for NRS back pain. The estimated cut-offs were similar for LSS and for LDS.
Conclusion: For estimating a 'success' rate assessed by a PROM, we recommend using the follow-up score or the percentage change score. These scores reflected a clinically important outcome better than the change score.
Keywords: Back pain; Leg pain; Lumbar degenerative spondylolisthesis (LDS); Lumbar spinal stenosis (LSS); Minimal clinically important difference (MCID); Oswestry disability index (ODI); Patient reported outcome measures (PROMs); Success criteria.
Conflict of interest statement
Ethics approval and consent to participate
All patients have signed an informed consent form.
The protocol has been approved by the Norwegian Committee for Medical and Health Research Ethics Midt (2014/344).
Consent for publication
Not applicable.
Competing interests
None of the authors have any conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, Coumans JV, Harrington JF, Amin-Hanjani S, Schwartz JS, Sonntag VK, Barker FG, 2nd, Benzel EC. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. NEJM. 2016;374:1424–1434. doi: 10.1056/NEJMoa1508788. - DOI - PubMed
-
- Watters WC, 3rd, Baisden J, Gilbert TJ, Kreiner S, Resnick DK, Bono CM, Ghiselli G, Heggeness MH, Mazanec DJ, O'Neill C, Reitman CA, Shaffer WO, Summers JT, Toton JF. Degenerative lumbar spinal stenosis: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis. Spine J. 2008;8:305–310. doi: 10.1016/j.spinee.2007.10.033. - DOI - PubMed
-
- Weinstein JN, Lurie JD, Tosteson TD, Hanscom B, Tosteson AN, Blood EA, Birkmeyer NJ, Hilibrand AS, Herkowitz H, Cammisa FP, Albert TJ, Emery SE, Lenke LG, Abdu WA, Longley M, Errico TJ, Hu SS. Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. NEJM. 2007;356:2257–2270. doi: 10.1056/NEJMoa070302. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
