

Are blood lipids associated with microvascular complications among type 2 diabetes mellitus patients? A cross-sectional study in Shanghai, China
- PMID: 30658647
- PMCID: PMC6339385
- DOI: 10.1186/s12944-019-0970-2
Are blood lipids associated with microvascular complications among type 2 diabetes mellitus patients? A cross-sectional study in Shanghai, China
Abstract
Background: Although there are several studies to investigate the association between blood lipids and microvascular complications, these studies reported conflicting results. The aim of the current study was to explore the association between blood lipid parameters and the risk of microvascular complications, especially the dose-response association between them, among community patients with type 2 diabetes mellitus (T2DM) in Shanghai, China.
Methods: The cross-sectional study was conducted in 6 community health service centers in Shanghai between December 2014 and December 2016.The associations between blood lipids and diabetic kidney disease (DKD) or diabetic retinopathy (DR) were assessed using multiple logistic regression. Restricted cubic spline (RCS) was employed to estimate the dose-response relation of blood lipids and the risk of microvascular complications.
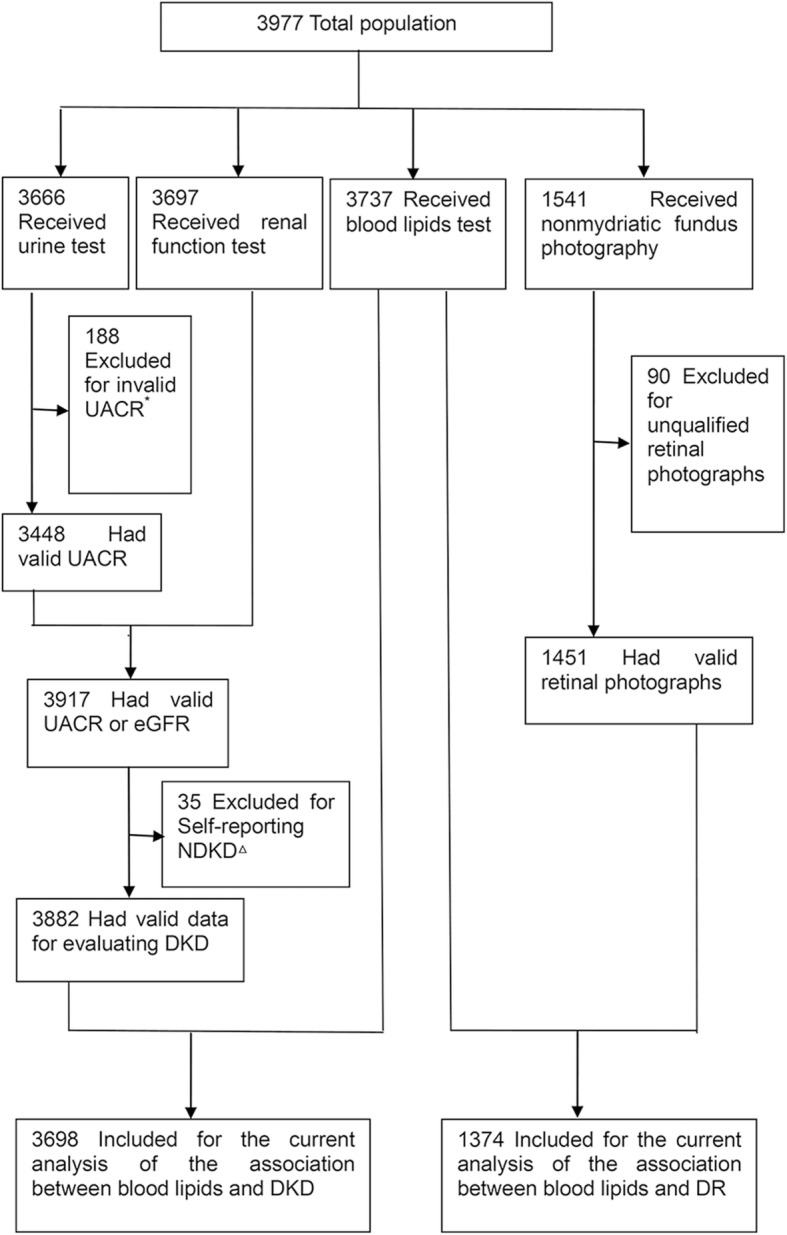
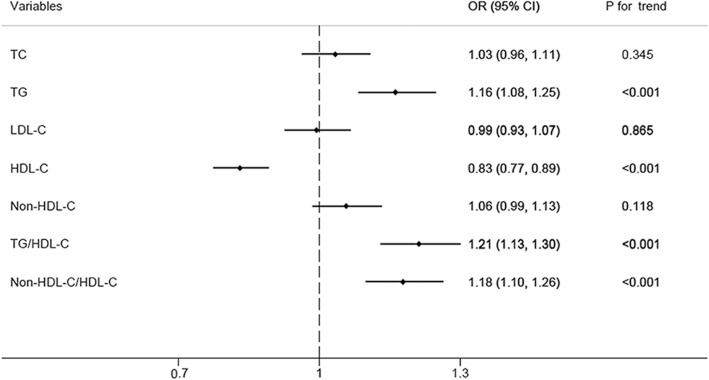
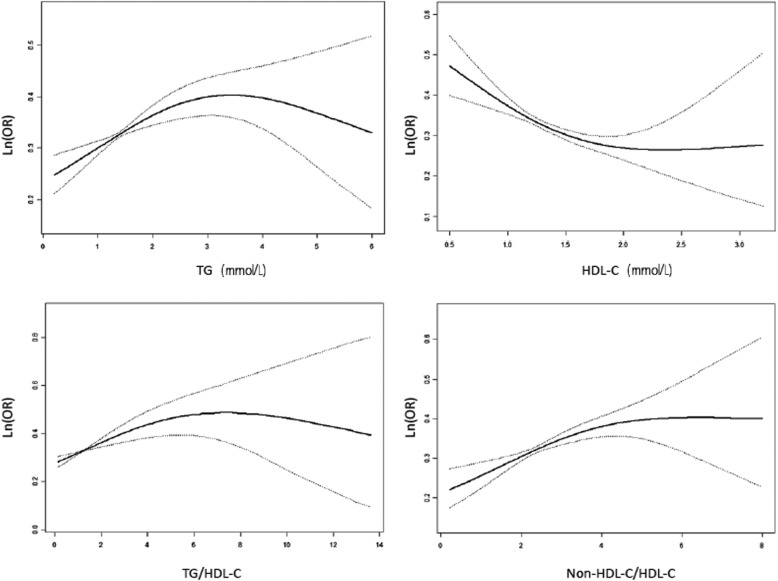
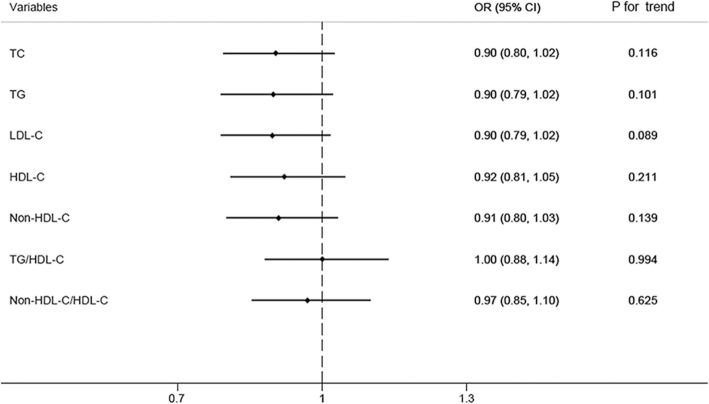
Results: A total of 3698 participants were included in the final analysis to study the association between blood lipids and DKD, wherein 33.2% of participants had DKD and 1374 were included for the analysis of the association between blood lipids and DR, wherein 23.2% of participants had DR. DKD odds ratio was increased by 1.16(95%CI,1.08-1.25), 1.21(95%CI,1.13-1.30), 1.18(95%CI,1.10-1.26) for comparing fourth to first quartiles of triglycerides (TG), TG/high-density lipoprotein cholesterol (HDL-C), non-HDL-C/HDL-C, respectively, and decreased by 0.83(95%CI,0.78-0.89) for comparing fourth to first quartiles of HDL-C. Furthermore, the dose-response association between TG, HDL-C, TG/HDL-C, non-HDL-C/HDL-C and the risk of DKD demonstrated turning points in TG of 1.90 mmol/L, HDL-C of 1.62 mmol/L, TG/HDL-C of 2.00, non-HDL-C/HDL-C of 3.09, respectively. However, no significant association was found between blood lipid parameters and DR.
Conclusions: This community-based study indicated that TG, HDL-C, TG/HDL-C, non-HDL-C/HDL-C were independently associated with DKD but not DR.
Keywords: Blood lipids; Diabetic kidney disease; Diabetic retinopathy; Type 2 diabetes mellitus.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Zhongshan Hospital of Fudan University (B2016–029). Written informed consent was obtained from all the participants.
Consent for publication
Written informed consent was obtained to publish from all the participants to report individual patient data.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The impact of serum lipids on risk for microangiopathy in patients with type 2 diabetes mellitus.Cardiovasc Diabetol. 2012 Sep 14;11:109. doi: 10.1186/1475-2840-11-109. Cardiovasc Diabetol. 2012. PMID: 22978715 Free PMC article.
-
A cohort study on the risk of diabetic retinopathy in type 2 diabetes patients with serum TG/HDL-C ratio.Prim Care Diabetes. 2025 Apr;19(2):195-200. doi: 10.1016/j.pcd.2025.01.005. Epub 2025 Jan 31. Prim Care Diabetes. 2025. PMID: 39893093
-
Association between plasma triglycerides and high-density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: a global case-control study in 13 countries.Circulation. 2014 Mar 4;129(9):999-1008. doi: 10.1161/CIRCULATIONAHA.113.002529. Epub 2013 Dec 18. Circulation. 2014. PMID: 24352521
-
Lipid variability and risk of microvascular complications in patients with diabetes: a systematic review and meta-analysis.BMC Endocr Disord. 2024 Jan 2;24(1):4. doi: 10.1186/s12902-023-01526-9. BMC Endocr Disord. 2024. PMID: 38167035 Free PMC article.
-
Probiotics improve renal function, glucose, lipids, inflammation and oxidative stress in diabetic kidney disease: a systematic review and meta-analysis.Ren Fail. 2022 Dec;44(1):862-880. doi: 10.1080/0886022X.2022.2079522. Ren Fail. 2022. PMID: 35611435 Free PMC article.
Cited by
-
Prevalence of and factors related to microvascular complications in patients with type 2 diabetes mellitus in Tianjin, China: a cross-sectional study.Ann Transl Med. 2019 Jul;7(14):325. doi: 10.21037/atm.2019.06.08. Ann Transl Med. 2019. PMID: 31475195 Free PMC article.
-
Achievement of glycaemic control is associated with improvements in lipid profile with iGlarLixi versus iGlar: A post hoc analysis of the LixiLan-L trial.Diabetes Obes Metab. 2019 Dec;21(12):2712-2717. doi: 10.1111/dom.13857. Epub 2019 Sep 3. Diabetes Obes Metab. 2019. PMID: 31423722 Free PMC article. Clinical Trial.
-
Elevated waist-to-hip ratio, as an abdominal obesity index, predicts the risk of diabetic kidney injury.World J Diabetes. 2025 Apr 15;16(4):101384. doi: 10.4239/wjd.v16.i4.101384. World J Diabetes. 2025. PMID: 40236864 Free PMC article.
-
Both LDL and HDL particle concentrations associate positively with an increased risk of developing microvascular complications in patients with type 2 diabetes: lost protection by HDL (Zodiac-63).Cardiovasc Diabetol. 2023 Jul 6;22(1):169. doi: 10.1186/s12933-023-01909-1. Cardiovasc Diabetol. 2023. PMID: 37415152 Free PMC article.
-
Poor Control of Plasma Triglycerides Is Associated with Early Decline of Estimated Glomerular Filtration Rates in New-Onset Type 2 Diabetes in China: Results from a 3-Year Follow-Up Study.J Diabetes Res. 2020 Sep 28;2020:3613041. doi: 10.1155/2020/3613041. eCollection 2020. J Diabetes Res. 2020. PMID: 33062710 Free PMC article.
References
-
- Xiao Y, Sui BY, Zhao K. Epidemiological features of the end-stage renal disease and the application, cost and payment of dialysis care in China. Chinese Journal of Health Policy. 2011;05:29–33.
MeSH terms
Substances
Grants and funding
- S15027/Project of Shanghai Foundation for Senior Citizens
- 12GWZX1001/Construction Project of Key Discipline of Public Health in Shanghai
- PW2015C-25/Science and Technology Project of Pudong New Area Commission of Health and Family Planning
- 2015ZB0601/Shanghai Municipal Commission of Health and Family Planning, Key Developing Disciplines
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
