

Vascular endothelial cadherin shedding is more severe in sepsis patients with severe acute kidney injury
- PMID: 30658667
- PMCID: PMC6339439
- DOI: 10.1186/s13054-019-2315-y
Vascular endothelial cadherin shedding is more severe in sepsis patients with severe acute kidney injury
Abstract
Background: Vascular endothelial cadherin (VE-cadherin) is a membrane protein that is the major component of adherens junctions between endothelial cells. It is crucial for regulating vascular integrity, endothelial permeability, and angiogenesis. During inflammatory processes, VE-cadherin is shed into circulation (sVE-cadherin). Plasma sVE-cadherin is elevated in sepsis, malignancy, autoimmune diseases, and coronary atherosclerosis. However, the relationship between specific organ failures, especially severe acute kidney injury (AKI) defined by requirement for renal replacement therapy (AKI-RRT), and plasma sVE-cadherin levels in severe sepsis has not been well studied.
Methods: The present study is a prospective study of critically ill adults with sepsis and acute respiratory failure (age ≥ 18 years) enrolled in the Validating Acute Lung Injury markers for Diagnosis (VALID) study. Plasma sVE-cadherin was measured at study enrollment. Primary analysis focused on the association between sVE-cadherin levels and the development of AKI, AKI-RRT, other organ dysfunction as defined by Brussels organ failure scores, pulmonary versus non-pulmonary sepsis, acute respiratory distress syndrome (ARDS), and in-hospital mortality.
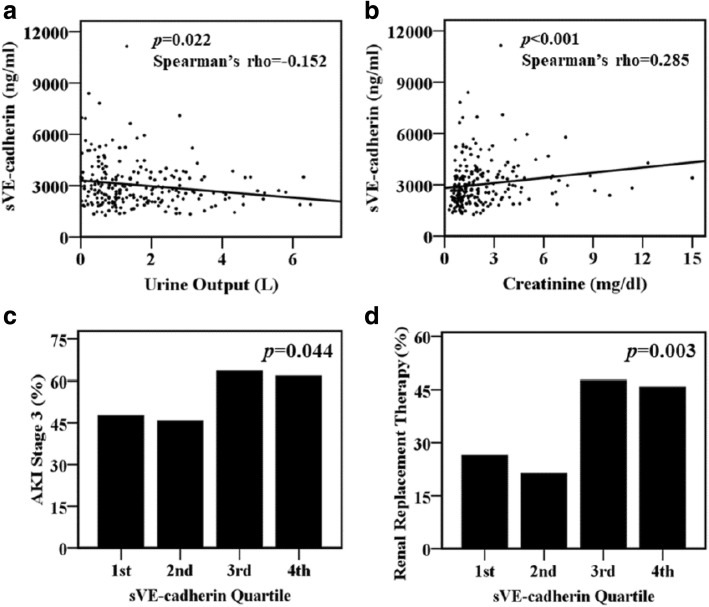
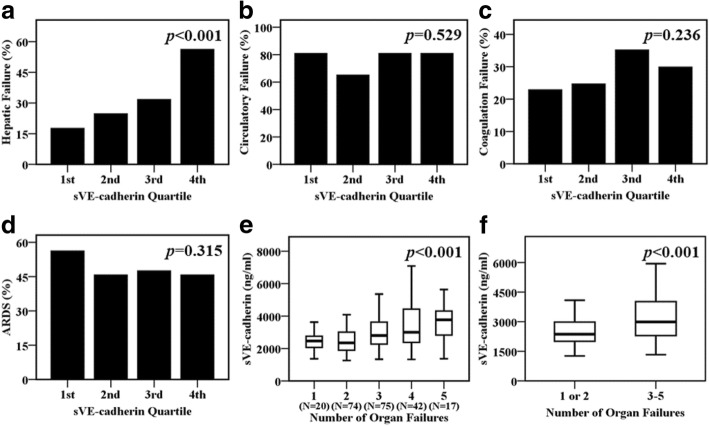
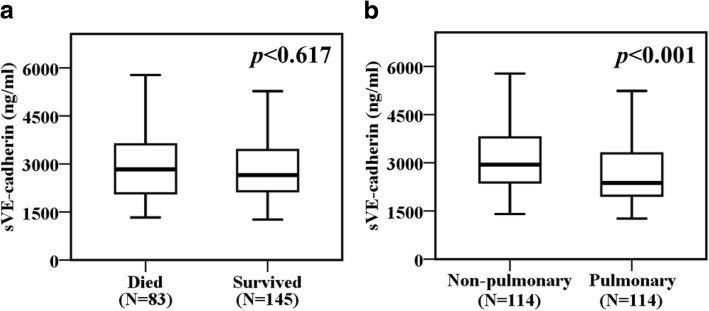
Results: Of 228 severe sepsis patients included, 80 (35%) developed AKI-RRT. Plasma sVE-cadherin levels at enrollment were significantly higher in patients with AKI-RRT compared with patients without AKI-RRT (p = 0.003). Plasma sVE-cadherin levels by quartile were significantly higher in severe sepsis patients with acute kidney injury stage 3 (p = 0.044) as defined by Kidney Disease Improving Global Outcomes (KDIGO) criteria. Patients with greater than 2 organ failures had higher plasma sVE-cadherin levels than patients with 2 or fewer organ failures (p < 0.001). In a multivariable analysis, plasma sVE-cadherin was independently associated with AKI-RRT (odds ratio 6.44 per log increase in plasma sVE-cadherin, 95% CI 1.126-36.847, p = 0.036). Plasma sVE-cadherin levels were significantly higher in patients with non-pulmonary sepsis compared to pulmonary sepsis (p < 0.001).
Conclusion: Shedding of sVE-cadherin is associated with severe acute kidney injury and with more severe organ dysfunction in patients with sepsis, suggesting that breakdown of endothelial adherens junctions may contribute to the pathogenesis of organ dysfunction in sepsis. Further studies of sVE-cadherin as a biomarker of disease severity in clinical sepsis are needed to better elucidate the role of VE-cadherin shedding in sepsis-induced severe organ dysfunction.
Keywords: Acute kidney injury; Endothelial injury; Renal replacement therapy; Sepsis; Soluble vascular endothelial cadherin.
Conflict of interest statement
Ethics approval and consent to participate
The prospective study was approved by Vanderbilt Institutional Review Board (IRB #051065). Informed consent was obtained for sample collection from the patients or surrogates whenever possible; if patients or surrogates were unable to provide consent, the institutional review board granted a waiver of consent due to the minimal risk nature of the study.
Consent for publication
not applicable
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Soluble vascular endothelial cadherin: a promising marker of critical illness?Crit Care. 2019 Feb 19;23(1):57. doi: 10.1186/s13054-019-2343-7. Crit Care. 2019. PMID: 30782198 Free PMC article. No abstract available.
-
Letter in response to "Vascular endothelial cadherin shedding is more severe in sepsis patients with severe acute kidney injury".Crit Care. 2019 May 14;23(1):167. doi: 10.1186/s13054-019-2455-0. Crit Care. 2019. PMID: 31088576 Free PMC article. No abstract available.
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- R01 HL135849/HL/NHLBI NIH HHS/United States
- HL135849/HL/NHLBI NIH HHS/United States
- HL103836/HL/NHLBI NIH HHS/United States
- Taipei Veterans General Hospital-National Yang-Ming University Excellent Physician Scientists Cultivation Program/National Yang-Ming University
- K08 HL136888/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
