

The effects of TNF-alpha inhibitor therapy on the incidence of infection in JIA children: a meta-analysis
- PMID: 30658717
- PMCID: PMC6339290
- DOI: 10.1186/s12969-019-0305-x
The effects of TNF-alpha inhibitor therapy on the incidence of infection in JIA children: a meta-analysis
Abstract
Background: Juvenile Idiopathic arthritis (JIA) is the most common chronic rheumatic disease in childhood. The diagnosis is based on the underlying symptoms of arthritis with an exclusion of other diseases Biologic agents are increasingly used on the side of disease-modifying anti-rheumatic drugs (DMARD) in JIA treatment.
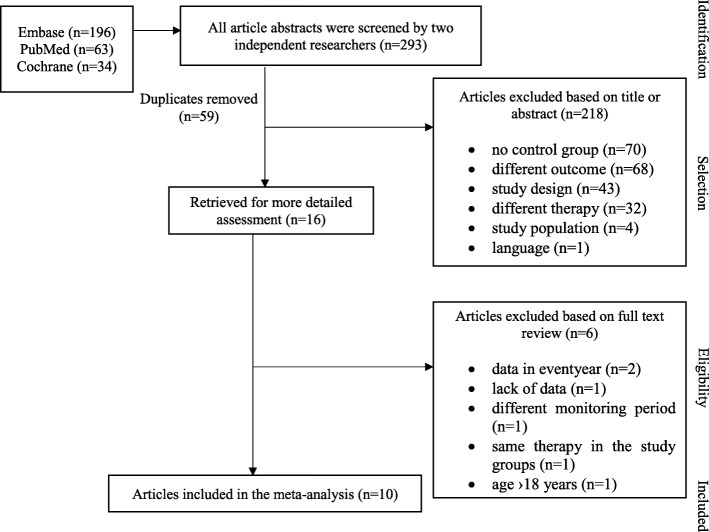
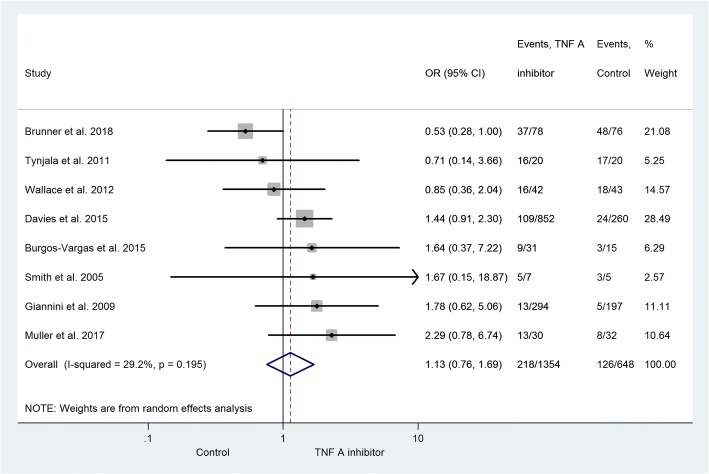
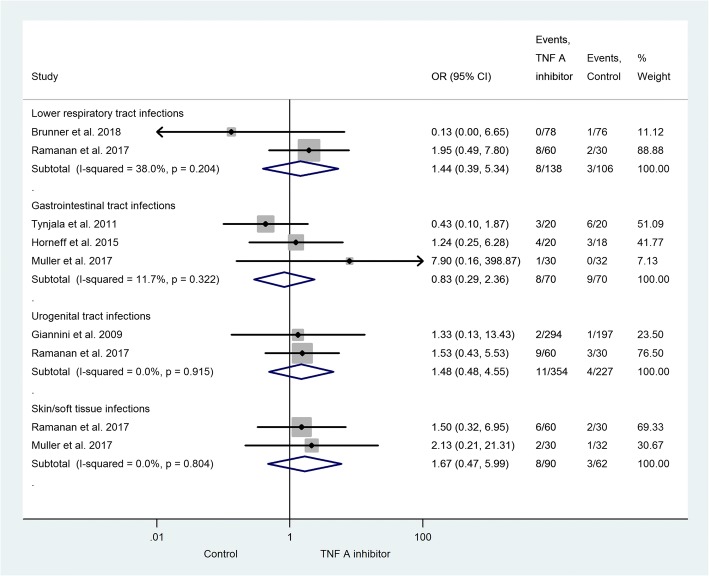
Main body: The aim of this meta-analysis was to investigate the observed infections in JIA children during tumor necrosis factor (TNF)-alpha inhibitor therapy. A systematic search of three databases (Medline via PubMed, Embase, Cochrane Library) was carried out up to May 2018. Published trials that evaluated the infectious adverse events in patients receiving TNF-alpha inhibitor vs. a control group were included in the analysis. Full-text data extraction was carried out independently by the investigators from ten relevant publications. 1434 patients received TNF-alpha inhibitor therapy; the control group consisted of 696 subjects. The analysis presented the risk of infection in the active treatment group (OR = 1.13; 95% CI: 0.76-1.69; p = 0.543). The majority of infections were upper respiratory tract infections (URTIs). Furthermore, the subgroup analysis demonstrated a higher infection rate in the observed localization.
Conclusion: Anti-TNF therapy slightly but not significantly increases the incidence of infection in JIA children compared to other therapies (GRADE: moderate evidence). The most common infections reported were mild URTIs. Further studies with larger patients number with a strong evidence level are crucially needed to finalize the answer whether anti-TNF therapy elevates and if yes on what extent the incidence of infection in JIA children.
Trial registration: Prospero: CRD42017067873 .
Keywords: DMARD; Infection; JIA; Placebo; TNF-alpha inhibitor.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Merino R, de Inocencio J, Garcia-Consuegra J. Evaluation of revised international league of associations for Rheumatology classification criteria for juvenile idiopathic arthritis in Spanish children (Edmonton 2001) J Rheumatol. 2005;32(3):559–561. - PubMed
-
- Beukelman T, Patkar NM, Saag KG, Tolleson-Rinehart S, Cron RQ, DeWitt EM, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features. Arthritis Care Res (Hoboken). 2011;63(4):465–482. doi: 10.1002/acr.20460. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
