

Mendelian Randomization Analysis of Hemoglobin A1c as a Risk Factor for Coronary Artery Disease
- PMID: 30659074
- PMCID: PMC6609962
- DOI: 10.2337/dc18-1712
Mendelian Randomization Analysis of Hemoglobin A1c as a Risk Factor for Coronary Artery Disease
Abstract
Objective: Observational studies show that higher hemoglobin A1c (A1C) predicts coronary artery disease (CAD). It remains unclear whether this association is driven entirely by glycemia. We used Mendelian randomization (MR) to test whether A1C is causally associated with CAD through glycemic and/or nonglycemic factors.
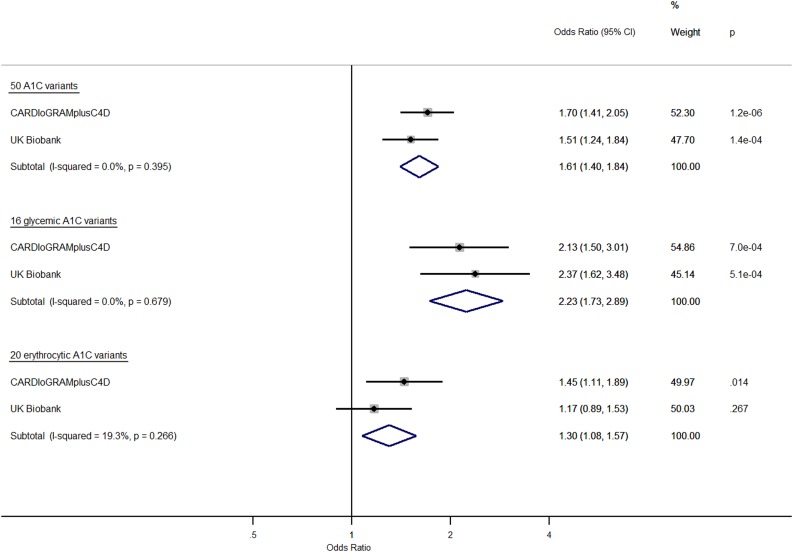
Research design and methods: To examine the association of A1C with CAD, we selected 50 A1C-associated variants (log10 Bayes factor ≥6) from an A1C genome-wide association study (GWAS; n = 159,940) and performed an inverse-variance weighted average of variant-specific causal estimates from CAD GWAS data (CARDIoGRAMplusC4D; 60,801 CAD case subjects/123,504 control subjects). We then replicated results in UK Biobank (18,915 CAD case subjects/455,971 control subjects) and meta-analyzed all results. Next, we conducted analyses using two subsets of variants, 16 variants associated with glycemic measures (fasting or 2-h glucose) and 20 variants associated with erythrocyte indices (e.g., hemoglobin [Hb]) but not glycemic measures. In additional MR analyses, we tested the association of Hb with A1C and CAD.
Results: Genetically increased A1C was associated with higher CAD risk (odds ratio [OR] 1.61 [95% CI 1.40, 1.84] per %-unit, P = 6.9 × 10-12). Higher A1C was associated with increased CAD risk when using only glycemic variants (OR 2.23 [1.73, 2.89], P = 1.0 × 10-9) and when using only erythrocytic variants (OR 1.30 [1.08, 1.57], P = 0.006). Genetically decreased Hb, with concomitantly decreased mean corpuscular volume, was associated with higher A1C (0.30 [0.27, 0.33] %-unit, P = 2.9 × 10-6) per g/dL and higher CAD risk (OR 1.19 [1.04, 1.37], P = 0.02).
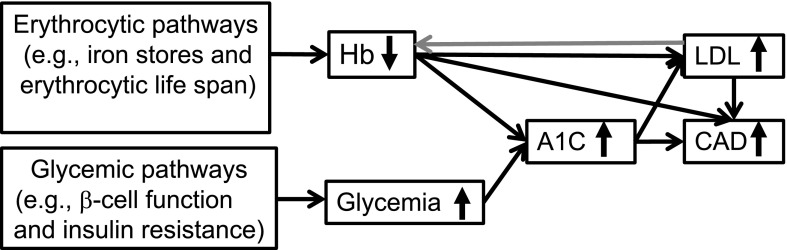
Conclusions: Genetic evidence supports a causal link between higher A1C and higher CAD risk. This relationship is driven not only by glycemic but also by erythrocytic, glycemia-independent factors.
© 2019 by the American Diabetes Association.
Figures
Comment in
-
Mediation of the Effect of Glycemia on the Risk of CVD Outcomes in Type 1 Diabetes: The DCCT/EDIC Study.Diabetes Care. 2019 Jul;42(7):1284-1289. doi: 10.2337/dc18-1613. Epub 2019 Mar 20. Diabetes Care. 2019. PMID: 30894365 Free PMC article.
-
The Cardiovascular Legacy of Good Glycemic Control: Clues About Mediators From the DCCT/EDIC Study.Diabetes Care. 2019 Jul;42(7):1159-1161. doi: 10.2337/dci19-0023. Diabetes Care. 2019. PMID: 31221692 No abstract available.
References
-
- Ross S, Gerstein HC, Eikelboom J, Anand SS, Yusuf S, Paré G. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes in the risk of coronary artery disease. Eur Heart J 2015;36:1454–1462 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
