

Clinical pathophysiology of thyroid eye disease: The Cone Model
- PMID: 30659242
- PMCID: PMC6367424
- DOI: 10.1038/s41433-018-0302-1
Clinical pathophysiology of thyroid eye disease: The Cone Model
Abstract
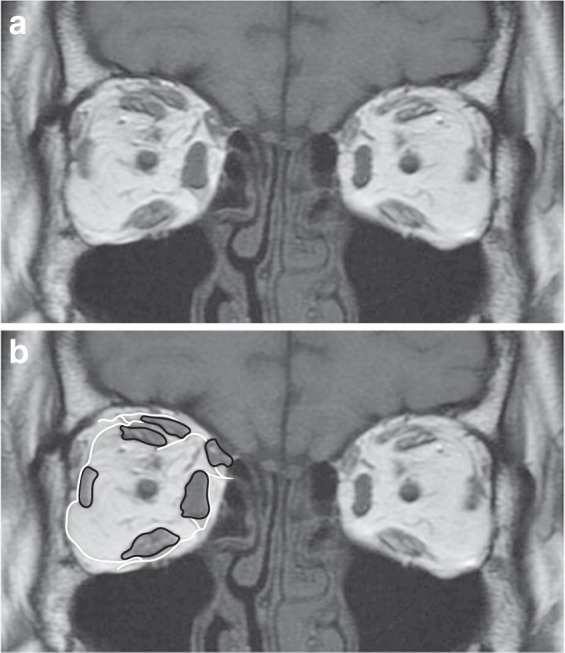
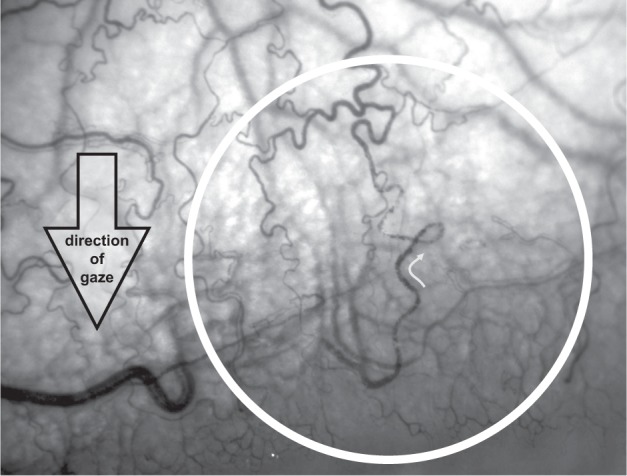
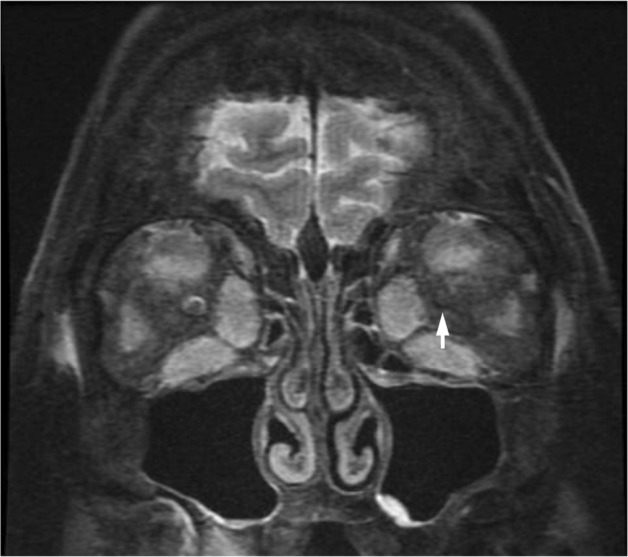
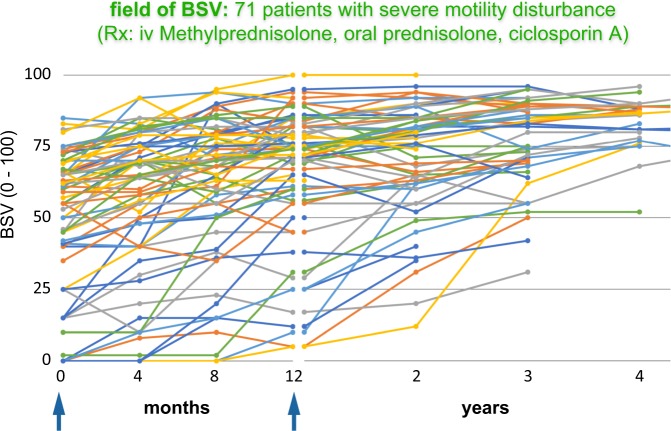
The clinical features of thyroid eye disease are dictated by the orbit's compartmentalisation; particularly, the muscle cone, which is delimited by the rectus muscles, their inter-muscular septa and the posterior sclera. The cone is anchored to the orbit apex and contains the posterior globe, the muscle bellies, a fat pad, and the blood circulation, optic nerve, and CSF sheath. It is surrounded by mobile extraconal fat, retained by the orbital septum.Thyroid eye disease is caused by expansion of muscle bellies and fat within the cone. Mechanical properties of the cone determine that the disease partitions into three phases: circumferential expansion, with forward displacement of extraconal fat; axial elongation, with increasing cone pressure; impedance of posterior venous outflow, with cone oedema and venous flow reversal.Venous flow reversal can be observed in the conjunctival circulation. It is initially transient, accompanying rises in cone pressure caused by eye movements, but later becomes permanent. It is a useful clinical sign that locates diseased muscles and anticipates venous compressive crises.Strabismus arises when inflamed rectus muscles, swollen by hydrated glycosaminoglycans, lose contractility and compliance. The incomitance is moderated by increasing stiffness affecting all the rectus muscles, as they are stretched during cone expansion.Immunomodulation, which rapidly reduces cone volume, relieving muscle elongation and stiffness, may paradoxically unmask strabismus. However, ciclosporin A suppresses late post-inflammatory fibrosis and only 4 of 71 patients so-treated required strabismus surgery.The cone model also accounts for the variety of clinical presentations of thyroid eye disease.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
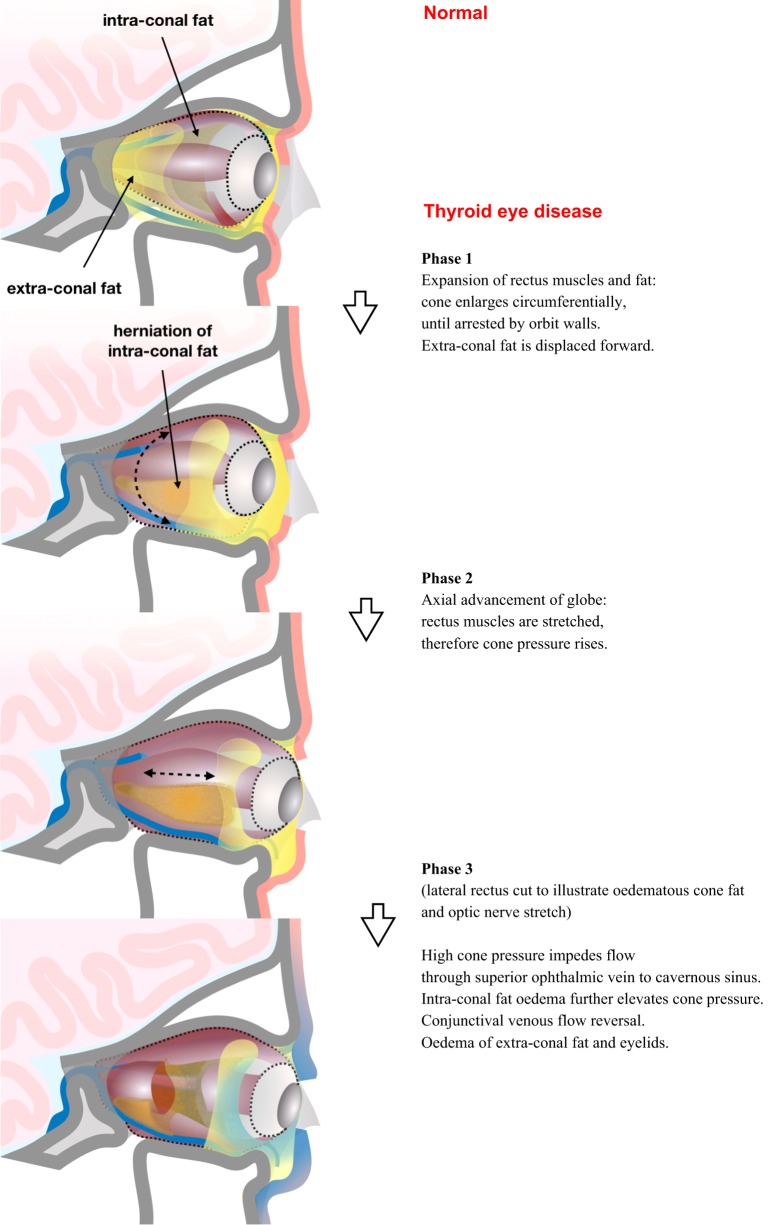
 . Venous drainage to the cavernous sinus passes both through the cone (superior ophthalmic vein) and outside it (inferior ophthalmic vein). The cone is surrounded by extraconal fat. Thyroid eye disease: 1/ circumferential enlargement of the muscle cone displaces extraconal fat; 2/ stretching of rectus muscles elevates cone pressure; 3/ high pressure impedes venous drainage to the cavernous sinus.
. Venous drainage to the cavernous sinus passes both through the cone (superior ophthalmic vein) and outside it (inferior ophthalmic vein). The cone is surrounded by extraconal fat. Thyroid eye disease: 1/ circumferential enlargement of the muscle cone displaces extraconal fat; 2/ stretching of rectus muscles elevates cone pressure; 3/ high pressure impedes venous drainage to the cavernous sinus.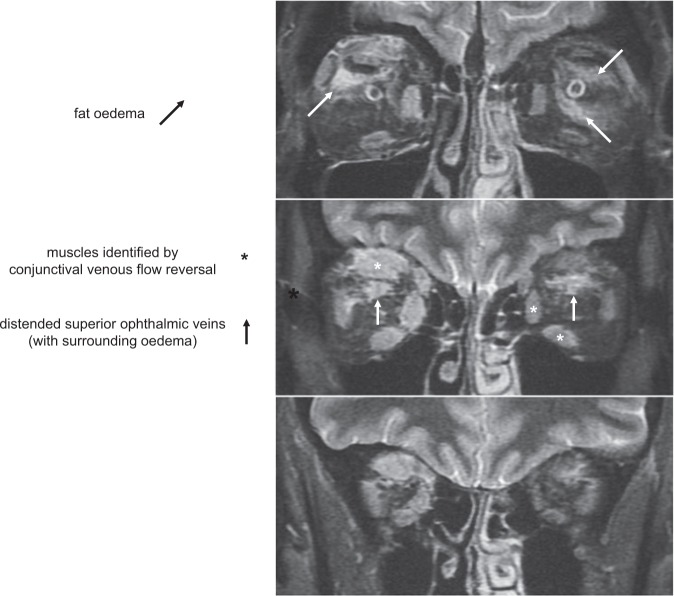

References
-
- Gordon JE. Structures. Penguin: UK, 1978.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
