

Feasibility of an alternative, physiologic, individualized open-lung approach to high-frequency oscillatory ventilation in children
- PMID: 30659380
- PMCID: PMC6338613
- DOI: 10.1186/s13613-019-0492-0
Feasibility of an alternative, physiologic, individualized open-lung approach to high-frequency oscillatory ventilation in children
Abstract
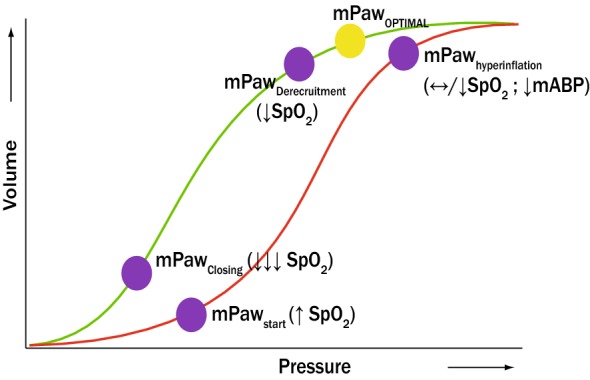
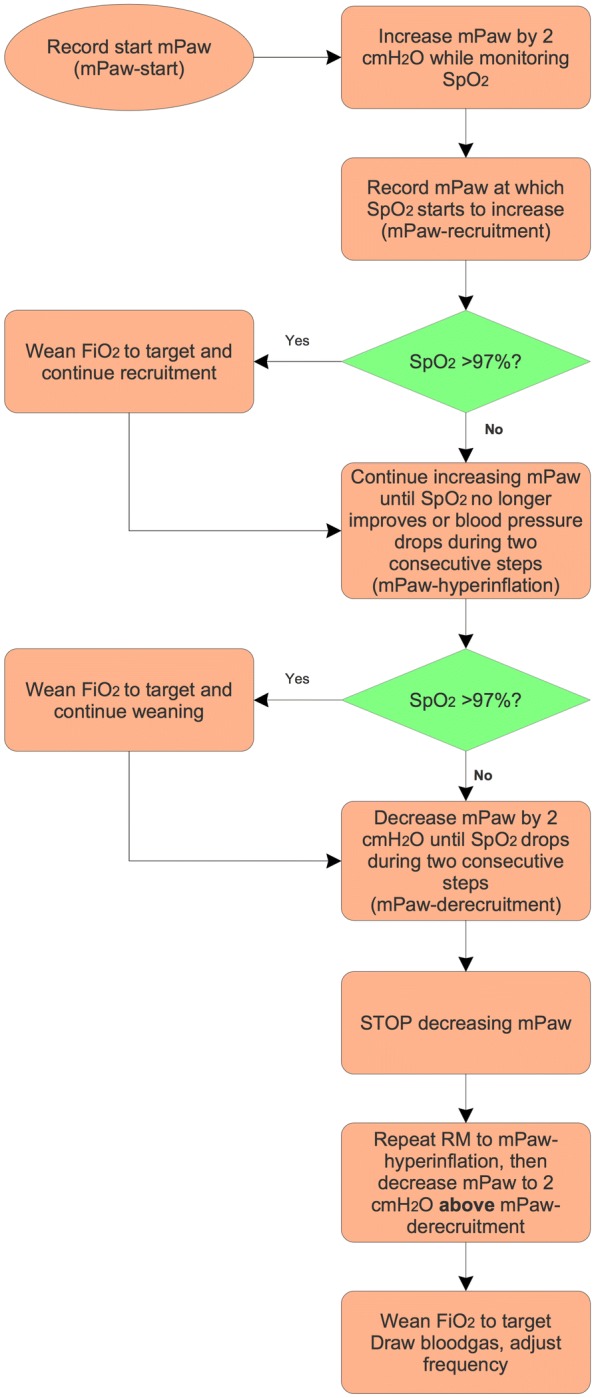
Background: High-frequency oscillatory ventilation (HFOV) is a common but unproven management strategy in paediatric critical care. Oscillator settings have been traditionally guided by patient age and/or weight rather than by lung mechanics, thereby potentially negating any beneficial effects. We have adopted an open-lung HFOV strategy based on a corner frequency approach using an initial incremental-decremental mean airway pressure titration manoeuvre, a high frequency (8-15 Hz), and high power to initially target a proximal pressure amplitude (∆Pproximal) of 70-90 cm H2O, irrespective of age or weight.
Methods: We reviewed prospectively collected data on patients < 18 years of age who were managed with HFOV for acute respiratory failure. We measured metrics for oxygenation, ventilation, and haemodynamics as well as the use of sedative-analgesic medications and neuromuscular blocking agents.
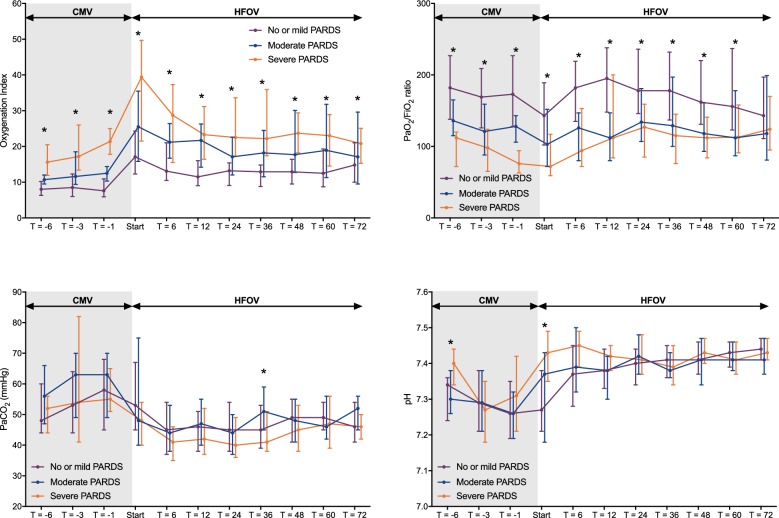
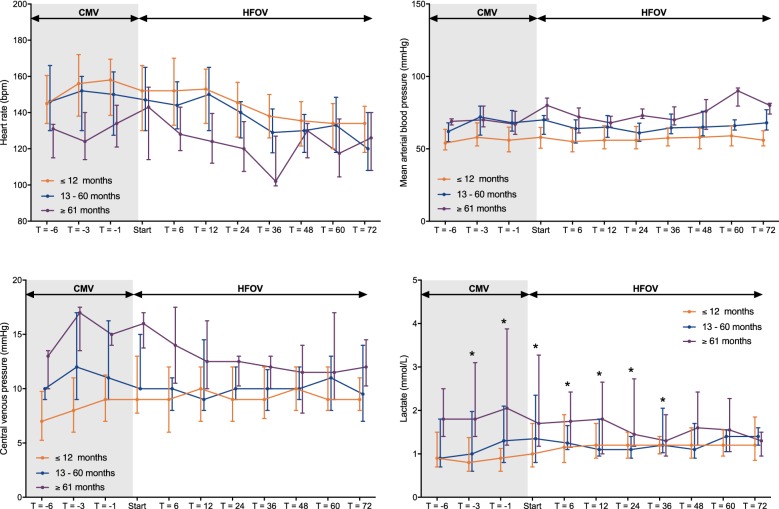
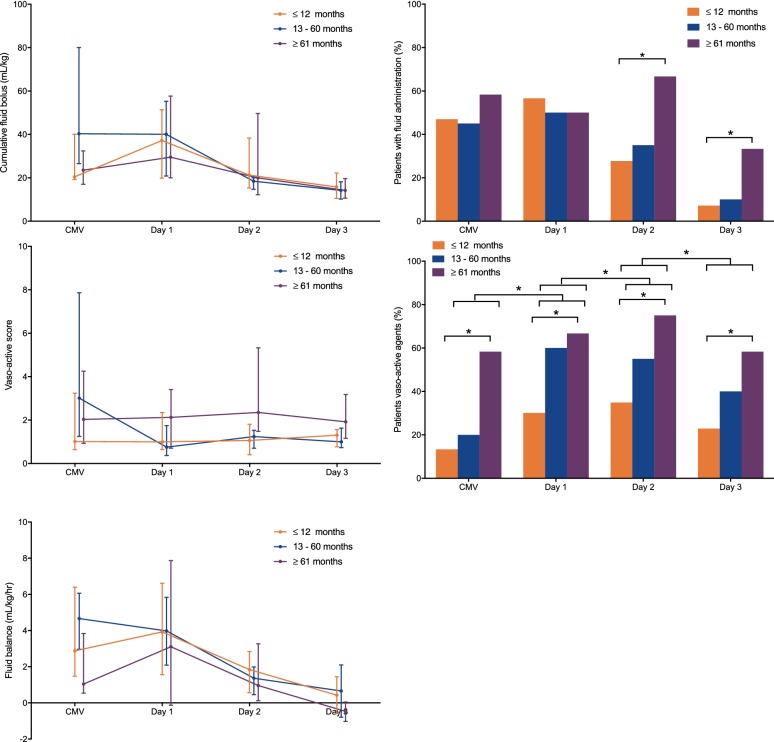
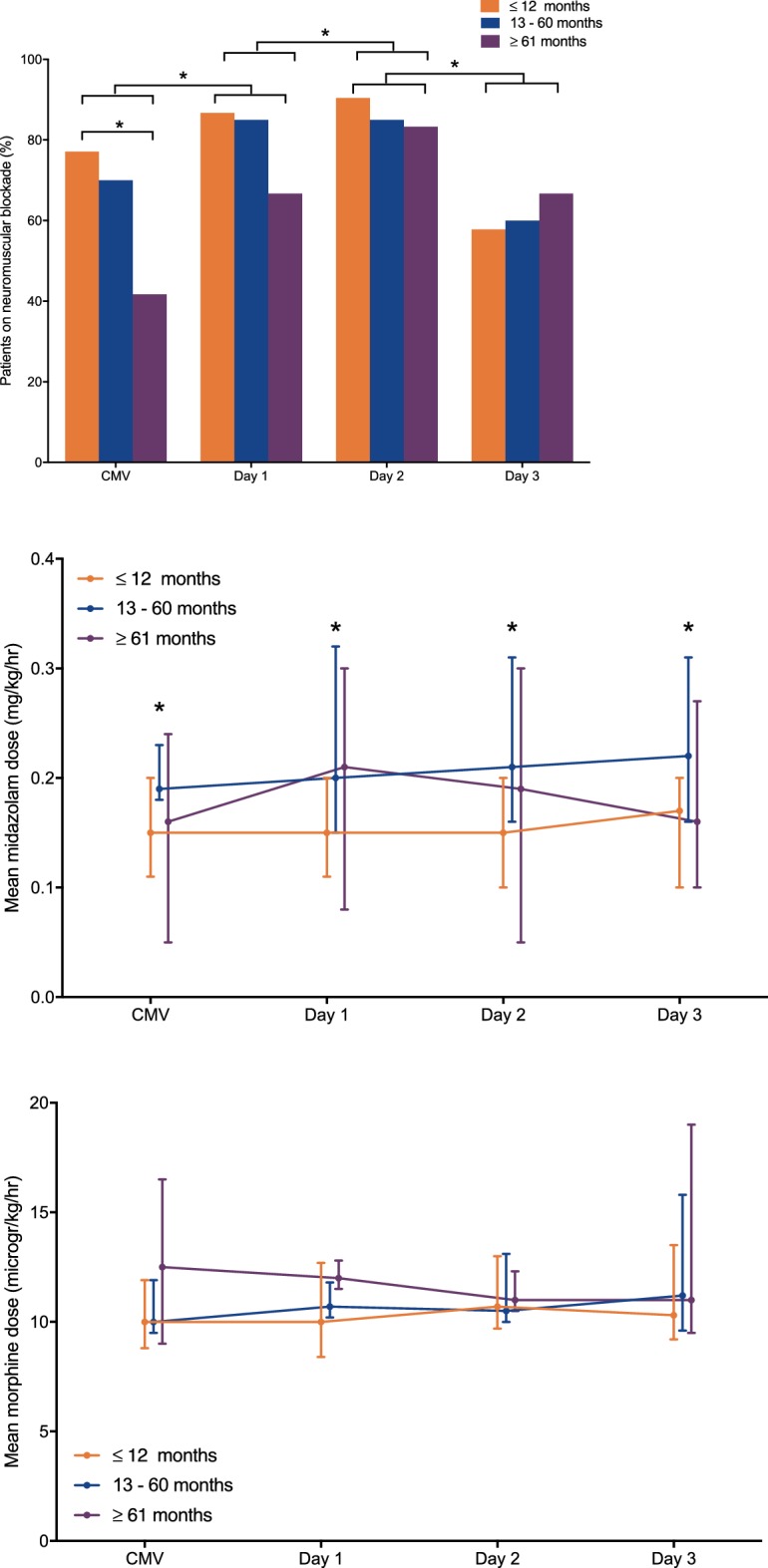
Results: Data from 115 non-cardiac patients were analysed, of whom 53 had moderate-to-severe paediatric acute respiratory distress syndrome (PARDS). Sixteen patients (13.9%) died. Frequencies≥ 8 Hz and high ∆Pproximal were achieved in all patients irrespective of age or PARDS severity. Patients with severe PARDS showed the greatest improvement in oxygenation. pH and PaCO2 normalized in all patients. Haemodynamic parameters, cumulative amount of fluid challenges, and daily fluid balance did not deteriorate after transitioning to HFOV in any age or PARDS severity group. We observed a transient increase neuromuscular blocking agent use after switching to HFOV, but there was no increase in the daily cumulative amount of continuous midazolam or morphine in any age or PARDS severity group. No patients experienced clinically apparent barotrauma.
Conclusions: This is the first study reporting the feasibility of an alternative, individualized, physiology-based open-lung HFOV strategy targeting high F and high ∆Pproximal. No adverse effects were observed with this strategy. Our findings warrant further systematic evaluation.
Keywords: Acute respiratory failure; Child; High-frequency oscillatory ventilation; Mechanical ventilation; Oxygenation; Paediatric acute respiratory distress syndrome; Paediatrics.
Figures

Similar articles
-
The impact of high frequency oscillatory ventilation on mortality in paediatric acute respiratory distress syndrome.Crit Care. 2020 Jan 31;24(1):31. doi: 10.1186/s13054-020-2741-x. Crit Care. 2020. PMID: 32005285 Free PMC article.
-
Effect of early intervention of high-frequency oscillatory ventilation on the outcome in pediatric acute respiratory distress syndrome.Bratisl Lek Listy. 2000;101(1):8-13. Bratisl Lek Listy. 2000. PMID: 10824405
-
Hemodynamic Effects of a High-Frequency Oscillatory Ventilation Open-Lung Strategy in Critically Ill Children With Acquired or Congenital Cardiac Disease.Pediatr Crit Care Med. 2023 Jun 1;24(6):e272-e281. doi: 10.1097/PCC.0000000000003211. Epub 2023 Mar 6. Pediatr Crit Care Med. 2023. PMID: 36877029 Free PMC article.
-
High-frequency oscillatory ventilation for acute respiratory distress syndrome in adult patients.Crit Care Med. 2003 Apr;31(4 Suppl):S317-23. doi: 10.1097/01.CCM.0000057910.50618.EB. Crit Care Med. 2003. PMID: 12682459 Review.
-
High-frequency oscillatory ventilation in adults with acute respiratory distress syndrome.Curr Opin Anaesthesiol. 2012 Feb;25(1):17-23. doi: 10.1097/ACO.0b013e32834ea57b. Curr Opin Anaesthesiol. 2012. PMID: 22157194 Review.
Cited by
-
Monitoring lung recruitability during recruitment maneuvers in children with respiratory failure on ECMO using electrical impedance tomography: case report.Front Pediatr. 2025 Feb 19;13:1545230. doi: 10.3389/fped.2025.1545230. eCollection 2025. Front Pediatr. 2025. PMID: 40046854 Free PMC article.
-
High-frequency oscillatory ventilation in a tertiary paediatric intensive care unit in an academic hospital in Johannesburg, South Africa.South Afr J Crit Care. 2019 Nov 1;35(2):10.7196/SAJCC.2019.v35i2.396. doi: 10.7196/SAJCC.2019.v35i2.396. eCollection 2019. South Afr J Crit Care. 2019. PMID: 37090029 Free PMC article.
-
Performance of acute respiratory distress syndrome definitions in a high acuity paediatric intensive care unit.Respir Res. 2021 Sep 29;22(1):256. doi: 10.1186/s12931-021-01848-z. Respir Res. 2021. PMID: 34587946 Free PMC article.
-
Physiologic responses to a staircase lung volume optimization maneuver in pediatric high-frequency oscillatory ventilation.Ann Intensive Care. 2020 Nov 18;10(1):153. doi: 10.1186/s13613-020-00771-8. Ann Intensive Care. 2020. PMID: 33206258 Free PMC article.
-
Acute Respiratory Distress Syndrome Management in Pediatric Intensive Care Units in Turkey: A Prospective Survey.Turk Arch Pediatr. 2022 Mar;57(2):216-221. doi: 10.5152/TurkArchPediatr.2022.21198. Turk Arch Pediatr. 2022. PMID: 35383018 Free PMC article.
References
-
- Arnold JH, Hanson JH, Toro-Figuero LO, Gutierrez J, Berens RJ, Anglin DL. Prospective, randomized comparison of high-frequency oscillatory ventilation and conventional mechanical ventilation in pediatric respiratory failure. Crit Care Med. 1994;22(10):1530–1539. doi: 10.1097/00003246-199422100-00006. - DOI - PubMed
LinkOut - more resources
Full Text Sources
