

Acute Microvascular Impairment Post-Reperfused STEMI Is Reversible and Has Additional Clinical Predictive Value: A CMR OxAMI Study
- PMID: 30660541
- PMCID: PMC6718360
- DOI: 10.1016/j.jcmg.2018.10.028
Acute Microvascular Impairment Post-Reperfused STEMI Is Reversible and Has Additional Clinical Predictive Value: A CMR OxAMI Study
Abstract
Objectives: This study sought to investigate the clinical utility and the predictive relevance of absolute rest myocardial blood flow (MBF) by cardiac magnetic resonance (CMR) in acute myocardial infarction.
Background: Microvascular obstruction (MVO) remains one of the worst prognostic factors in patients with reperfused ST-segment elevation myocardial infarction (STEMI). Clinical trials have focused on cardioprotective strategies to maintain microvascular functionality, but there is a need for a noninvasive test to determine their efficacy.
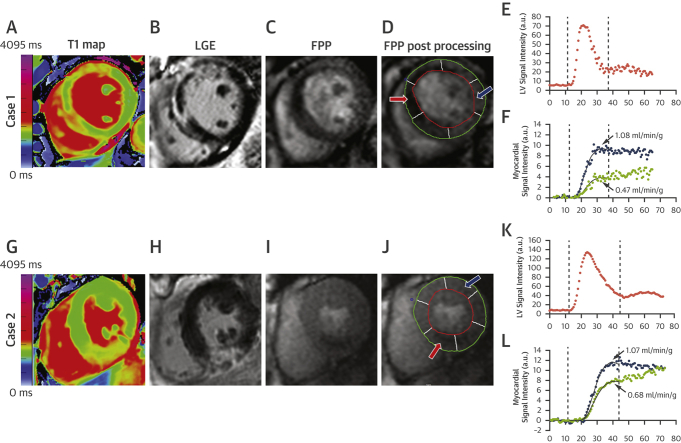
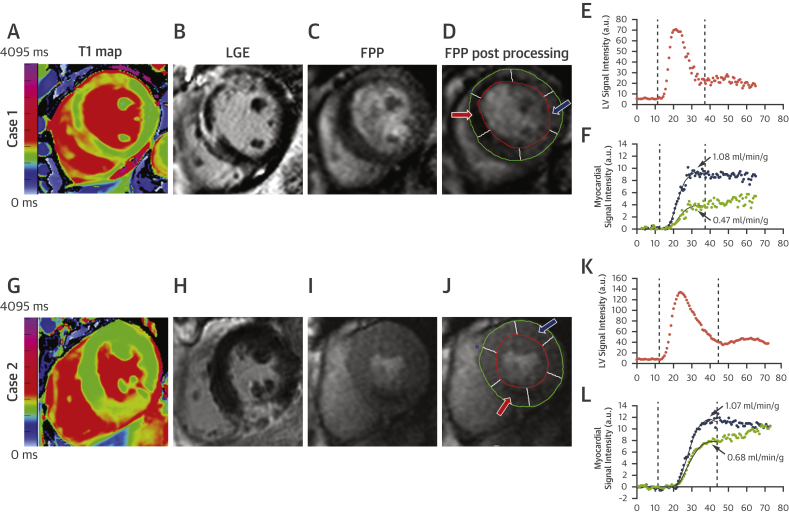
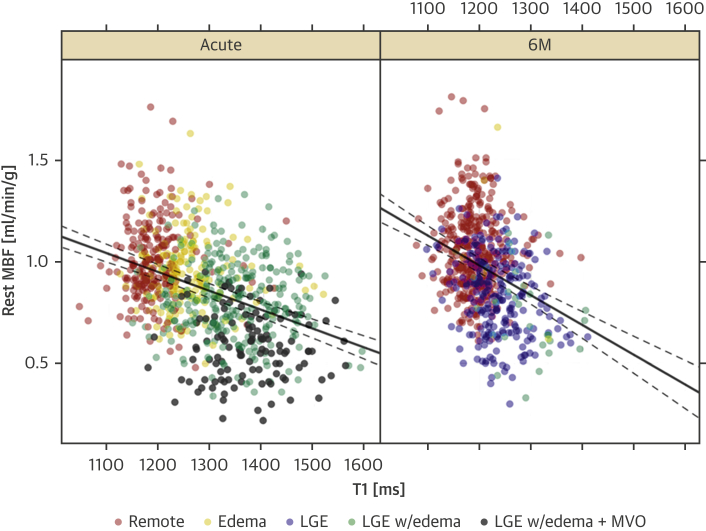
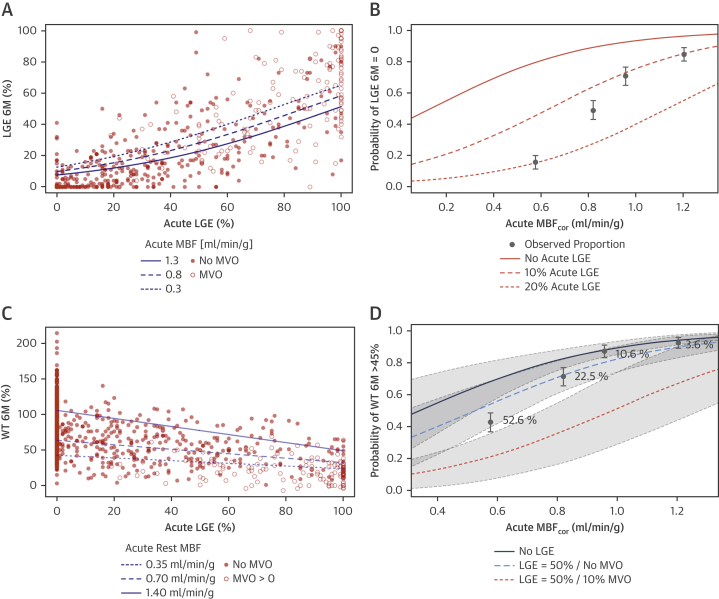
Methods: A total of 64 STEMI patients post-primary percutaneous coronary intervention underwent 3-T CMR scans acutely and at 6 months (6M). The protocol included cine function, T2-weighted edema imaging, pre-contrast T1 mapping, rest first-pass perfusion, and late gadolinium enhancement imaging. Segmental MBF, corrected for rate pressure product (MBFcor), was quantified in remote, edematous, and infarcted myocardium.
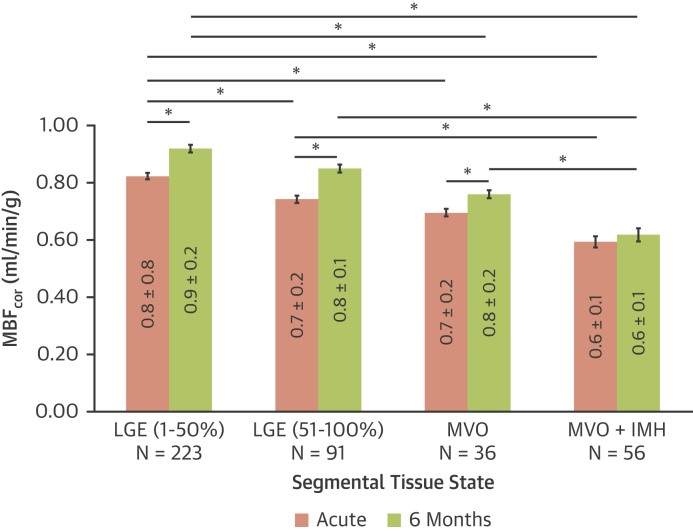
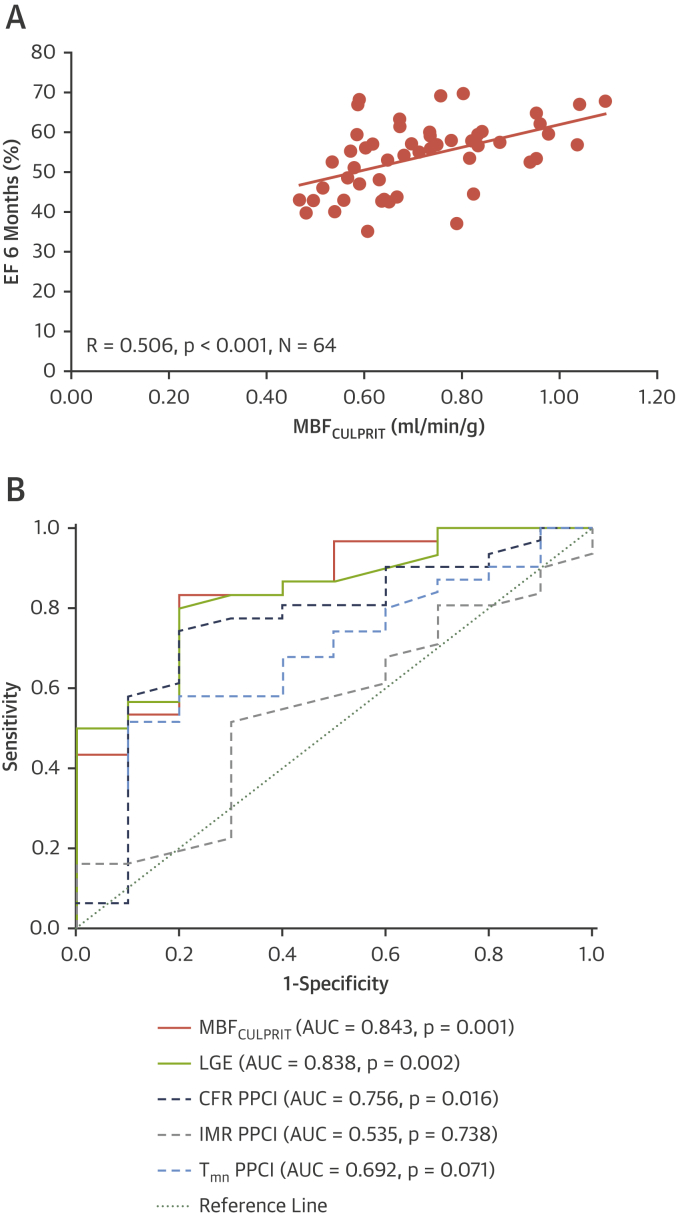
Results: Acute MBFcor was significantly reduced in infarcted myocardium compared with remote MBF (MBFinfarct 0.76 ± 0.20 ml/min/g vs. MBFremote 1.02 ± 0.21 ml/min/g, p < 0.001), but it significantly increased at 6M (MBFinfarct 0.76 ± 0.20 ml/min/g acute vs. 0.85 ± 0.22 ml/min/g at 6M, p < 0.001). On a segmental basis, acute MBFcor had incremental prognostic value for infarct size at 6M (odds of no LGE at 6M increased by 1.4:1 [p < 0.001] for each 0.1 ml/min/g increase of acute MBFcor) and functional recovery (odds of wall thickening >45% at 6M increased by 1.38:1 [p < 0.001] for each 0.1 ml/min/g increase of acute MBFcor). In subjects with coronary flow reserve >2 or index of myocardial resistance <40, acute MBF was associated with long-term functional recovery and was an independent predictor of infarct size reduction.
Conclusions: Acute MBF by CMR could represent a novel quantitative imaging biomarker of microvascular reversibility, and it could be used to identify patients who may benefit from more intensive or novel therapies.
Keywords: acute myocardial infarction; magnetic resonance; myocardial blood flow.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Myocardial Blood Flow as a Holistic Metric for Predicting Remodeling and Clinical Outcomes After a Myocardial Infarction?JACC Cardiovasc Imaging. 2019 Sep;12(9):1794-1796. doi: 10.1016/j.jcmg.2018.11.013. Epub 2019 Jan 16. JACC Cardiovasc Imaging. 2019. PMID: 30660548 No abstract available.
References
-
- de Waha S., Patel M.R., Granger C.B. Relationship between microvascular obstruction and adverse events following primary primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: an individual patient data pooled analysis from seven randomized trials. Eur Heart J. 2017;38:3502–3510. - PubMed
-
- Symons R., Pontone G., Schwitter J. Long-term incremental prognostic value of cardiovascular magnetic resonance after ST-segment elevation myocardial infarction. A study of the Collaborative Registry on CMR in STEMI. J Am Coll Cardiol Img. 2018;11:813–825. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
