

Epidemiology, Pathophysiology, and Treatment of Diverticulitis
- PMID: 30660732
- PMCID: PMC6716971
- DOI: 10.1053/j.gastro.2018.12.033
Epidemiology, Pathophysiology, and Treatment of Diverticulitis
Abstract
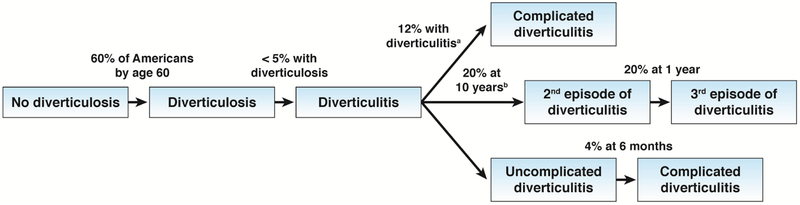
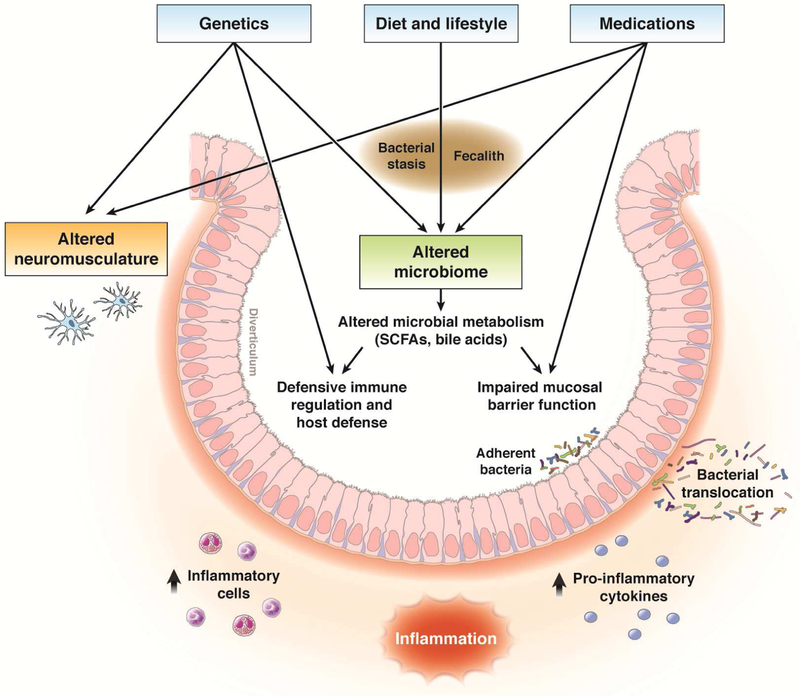
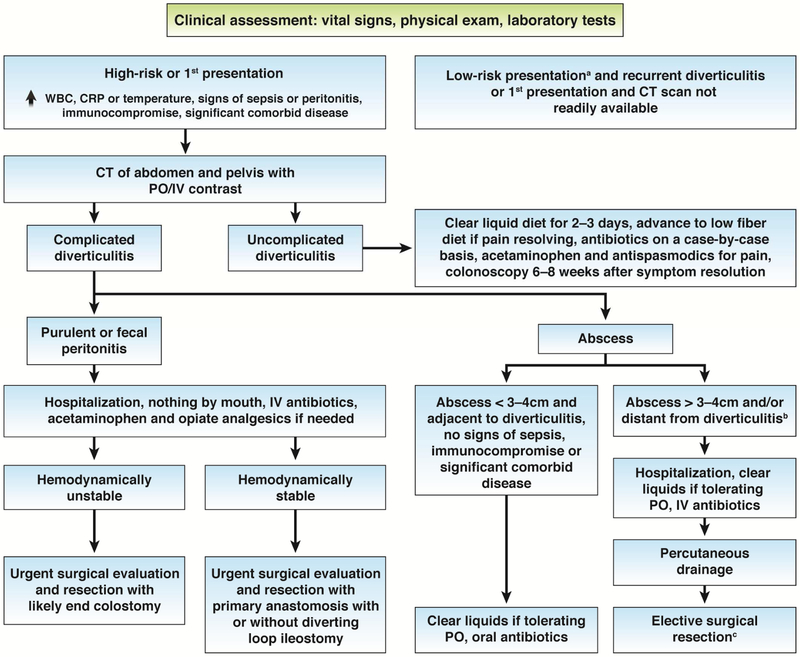
Diverticulitis is a prevalent gastrointestinal disorder that is associated with significant morbidity and health care costs. Approximately 20% of patients with incident diverticulitis have at least 1 recurrence. Complications of diverticulitis, such as abdominal sepsis, are less likely to occur with subsequent events. Several risk factors, many of which are modifiable, have been identified including obesity, diet, and physical inactivity. Diet and lifestyle factors could affect risk of diverticulitis through their effects on the intestinal microbiome and inflammation. Preliminary studies have found that the composition and function of the gut microbiome differ between individuals with vs without diverticulitis. Genetic factors, as well as alterations in colonic neuromusculature, can also contribute to the development of diverticulitis. Less-aggressive and more-nuanced treatment strategies have been developed. Two multicenter, randomized trials of patients with uncomplicated diverticulitis found that antibiotics did not speed recovery or prevent subsequent complications. Elective surgical resection is no longer recommended solely based on number of recurrent events or young patient age and might not be necessary for some patients with diverticulitis complicated by abscess. Randomized trials of hemodynamically stable patients who require urgent surgery for acute, complicated diverticulitis that has not improved with antibiotics provide evidence to support primary anastomosis vs sigmoid colectomy with end colostomy. Despite these advances, more research is needed to increase our understanding of the pathogenesis of diverticulitis and to clarify treatment algorithms.
Keywords: Chronic Manifestations; Functional Symptoms; Immunosuppression; Laparoscopic Lavage; Smoldering Diverticulitis.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Etzioni DA, Mack TM, Beart RW Jr., et al. Diverticulitis in the United States: 1998–2005: changing patterns of disease and treatment. Ann Surg 2009;249:210–7. - PubMed
-
- Regenbogen SE, Hardiman KM, Hendren S, et al. Surgery for diverticulitis in the 21st century: a systematic review. JAMA Surg 2014;149:292–303. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
