

Unexpected High Prevalence of Cardiovascular Disease Risk Factors and Psychiatric Disease Among Young People With Sudden Cardiac Arrest
- PMID: 30661423
- PMCID: PMC6497342
- DOI: 10.1161/JAHA.118.010330
Unexpected High Prevalence of Cardiovascular Disease Risk Factors and Psychiatric Disease Among Young People With Sudden Cardiac Arrest
Abstract
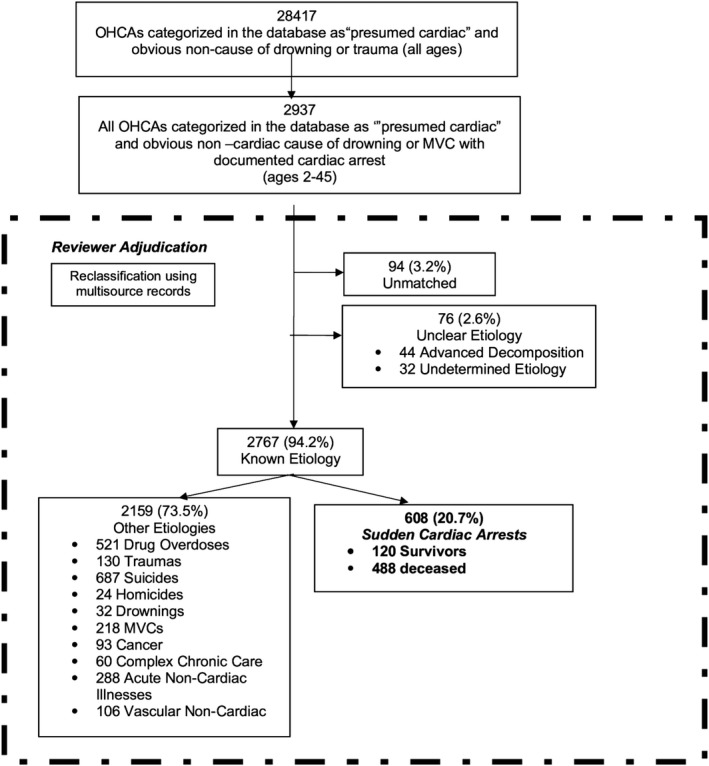
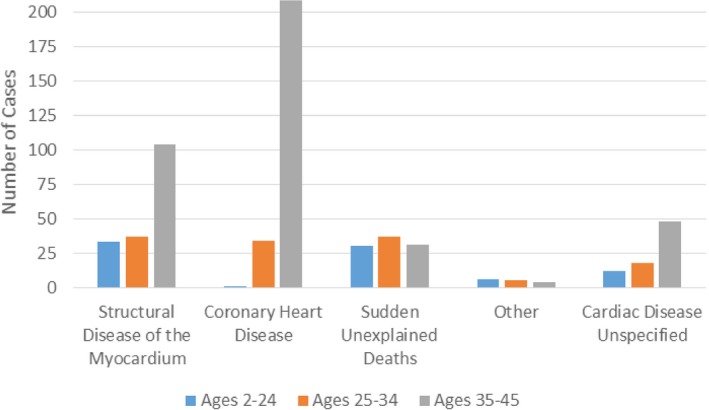
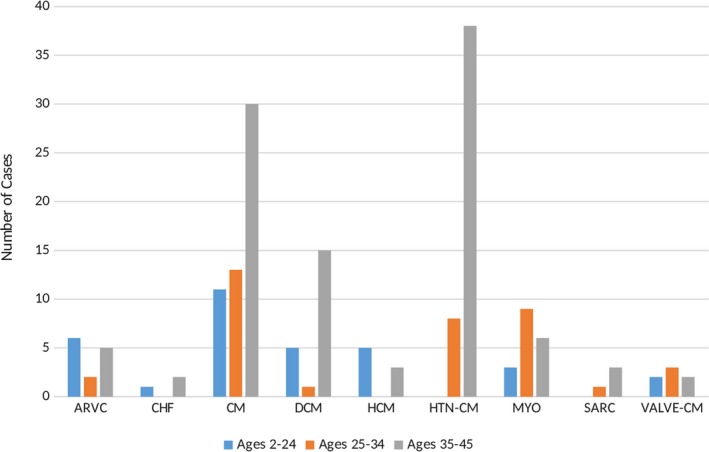
Background It is believed that most sudden cardiac arrests ( SCA s) in young people occur in previously healthy people with rare risk factors for sudden death. Few studies have investigated large populations with complete ascertainment. Our objective was to use multisource records to identify and classify all out-of-hospital cardiac arrests in the Greater Toronto Area (population 6.6 million) in people aged 2 to 45 years from 2009 to 2012. Methods and Results Expert reviewers employed a systematic process, with emergency medical services, in-hospital and coroner records, to adjudicate the cause of death as SCA from cardiac or noncardiac causes. We report the adjudicated etiologies, circumstances, triggers, and characteristics of the SCA cohort. Of 2937 eligible out-of-hospital cardiac arrest cases, 608 (20.7%) SCA s had an adjudicated etiology of cardiac cause (120 survivors and 488 nonsurvivors). Two thirds of these SCA patients had a history of cardiovascular disease, and over 50% had been diagnosed with ≥1 cardiovascular disease risk factor. Moreover, 20.1% of SCA s were diagnosed with psychiatric disease and 30% had central nervous system drugs prescribed. Over 30% of SCA patients had central nervous system active drugs, including drugs of abuse detected postmortem, with opioids and ethanol being detected most frequently. Potentially heritable structural cardiac diseases accounted for only 6.9% of SCA events, with acquired cardiac diseases comprising the rest. Conclusions The underlying causes of SCA , in people aged 2 to 45 years, often occur in those with previously diagnosed cardiovascular diseases, and are associated with contributory factors including prescribed medications, recreational drugs, and a concomitant psychiatric history.
Keywords: cardiovascular disease risk factors; etiology; psychiatric comorbidity; sudden cardiac arrest; sudden cardiac death; triggers; young.
Figures
Comment in
-
Sudden Cardiac Arrest in a Young Population: Not So Unpredictable.J Am Heart Assoc. 2019 Jan 22;8(2):e011700. doi: 10.1161/JAHA.118.011700. J Am Heart Assoc. 2019. PMID: 30663483 Free PMC article.
References
-
- Poirier P, Sharma S, Pipe A. The Atlantic Rift: guidelines for athletic screening‐where should Canada stand? Can J Cardiol. 2016;32:400–406. - PubMed
-
- Eckart RE, Shry EA, Burke AP, McNear JA, Appel DA, Castillo‐Rojas LM, Avedissian L, Pearse LA, Potter RN, Tremaine L, Gentlesk PJ, Huffer L, Reich SS, Stevenson WG; Department of Defense Cardiovascular Death Registry Group . Sudden death in young adults: an autopsy‐based series of a population undergoing active surveillance. J Am Coll Cardiol. 2011;58:1254–1261. - PubMed
-
- Winkel BG, Holst AG, Theilade J, Kristensen IB, Thomsen JL, Ottesen GL, Bundgaard H, Svendsen JH, Haunso S, Tfelt‐Hansen J. Nationwide study of sudden cardiac death in persons aged 1–35 years. Eur Heart J. 2011;32:983–990. - PubMed
-
- Wisten A, Forsberg H, Krantz P, Messner T. Sudden cardiac death in 15–35‐year olds in Sweden during 1992–99. J Intern Med. 2002;252:529–536. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
