

Personalized Prehospital Triage in Acute Ischemic Stroke
- PMID: 30661502
- PMCID: PMC6358183
- DOI: 10.1161/STROKEAHA.118.022562
Personalized Prehospital Triage in Acute Ischemic Stroke
Abstract
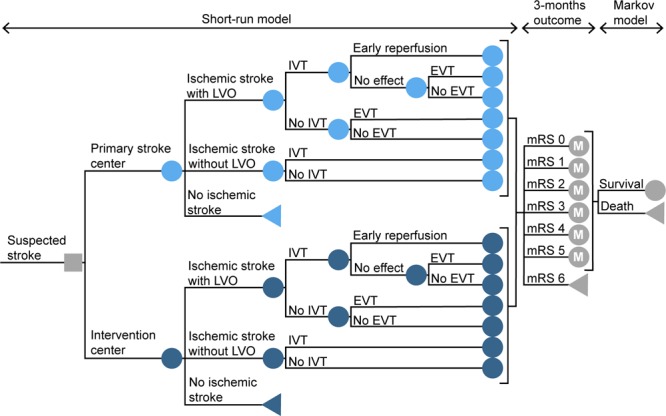
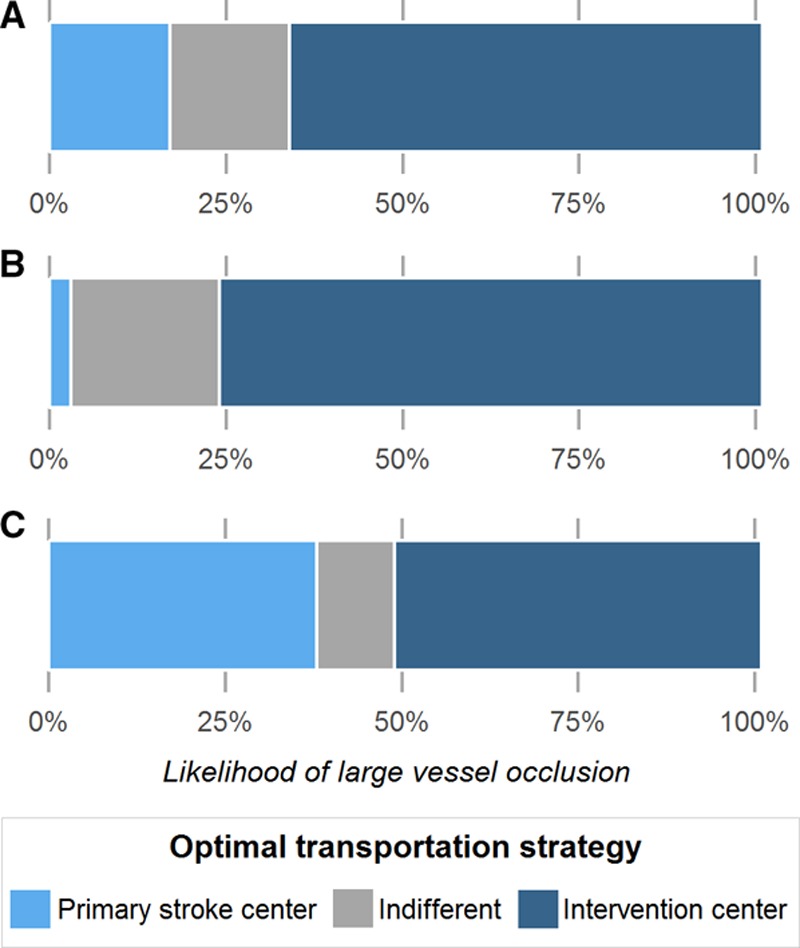
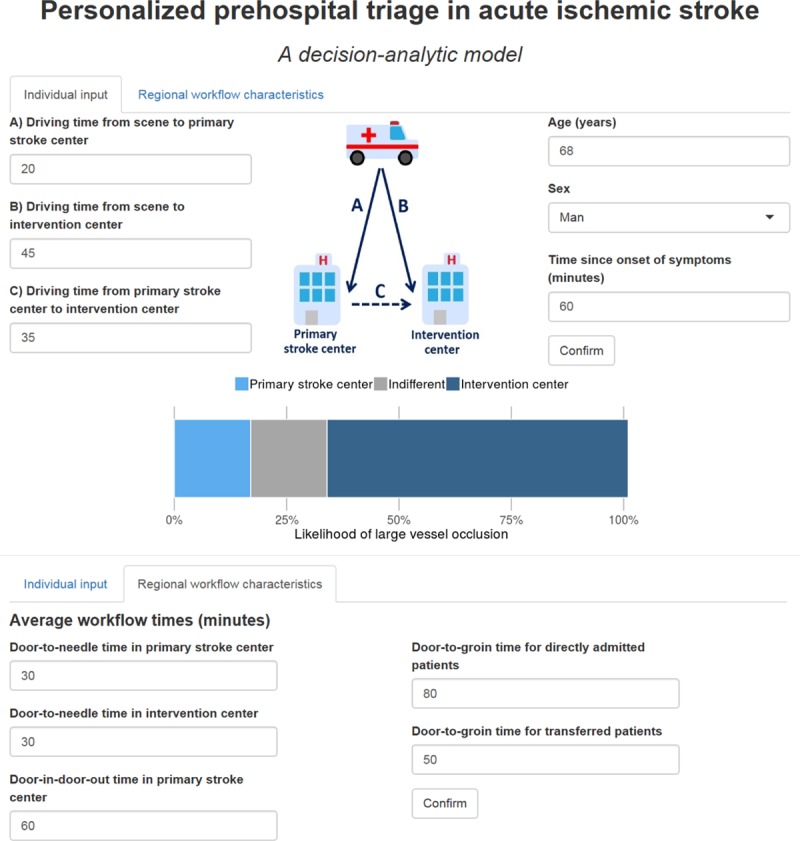
Background and Purpose- Direct transportation to a center with facilities for endovascular treatment might be beneficial for patients with acute ischemic stroke, but it can also cause harm by delay of intravenous treatment. Our aim was to determine the optimal prehospital transportation strategy for individual patients and to assess which factors influence this decision. Methods- We constructed a decision tree model to compare outcome of ischemic stroke patients after transportation to a primary stroke center versus a more distant intervention center. The optimal strategy was estimated based on individual patient characteristics, geographic location, and workflow times. In the base case scenario, the primary stroke center was located at 20 minutes and the intervention center at 45 minutes. Additional sensitivity analyses included an urban scenario (10 versus 20 minutes) and a rural scenario (30 versus 90 minutes). Results- Direct transportation to the intervention center led to better outcomes in the base case scenario when the likelihood of a large vessel occlusion as a cause of the ischemic stroke was >33%. With a high likelihood of large vessel occlusion (66%, comparable with a Rapid Arterial Occlusion Evaluation score of 5 or above), the benefit of direct transportation to the intervention center was 0.10 quality-adjusted life years (=36 days in full health). In the urban scenario, direct transportation to an intervention center was beneficial when the risk of large vessel occlusion was 24% or higher. In the rural scenario, this threshold was 49%. Other factors influencing the decision included door-to-needle times, door-to-groin times, and the door-in-door-out time. Conclusions- The preferred prehospital transportation strategy for suspected stroke patients depends mainly on the likelihood of large vessel occlusion, driving times, and in-hospital workflow times. We constructed a robust model that combines these characteristics and can be used to personalize prehospital triage, especially in more remote areas.
Keywords: decision tree; emergency medical services; quality-adjusted life years; thrombectomy; transportation.
Figures
References
-
- Goyal M, Jadhav AP, Bonafe A, Diener H, Mendes Pereira V, Levy E, et al. SWIFT PRIME investigators. Analysis of workflow and time to treatment and the effects on outcome in endovascular treatment of acute ischemic stroke: results from the SWIFT PRIME Randomized Controlled Trial. Radiology. 2016;279:888–897. doi: 10.1148/radiol.2016160204. - PubMed
-
- Menon BK, Sajobi TT, Zhang Y, Rempel JL, Shuaib A, Thornton J, et al. Analysis of workflow and time to treatment on thrombectomy outcome in the endovascular treatment for small core and proximal occlusion ischemic stroke (ESCAPE) Randomized, Controlled Trial. Circulation. 2016;133:2279–2286. doi: 10.1161/CIRCULATIONAHA.115.019983. - PubMed
-
- Menon BK, Almekhlafi MA, Pereira VM, Gralla J, Bonafe A, Davalos A, et al. STAR Study Investigators. Optimal workflow and process-based performance measures for endovascular therapy in acute ischemic stroke: analysis of the Solitaire FR thrombectomy for acute revascularization study. Stroke. 2014;45:2024–2029. doi: 10.1161/STROKEAHA.114.005050. - PubMed
-
- Venema E, Boodt N, Berkhemer OA, Rood PPM, van Zwam WH, van Oostenbrugge RJ, et al. MR CLEAN investigators. Workflow and factors associated with delay in the delivery of intra-arterial treatment for acute ischemic stroke in the MR CLEAN trial. J Neurointerv Surg. 2018;10:424–428. doi: 10.1136/neurintsurg-2017-013198. - PubMed
-
- Froehler MT, Saver JL, Zaidat OO, Jahan R, Aziz-Sultan MA, Klucznik RP, et al. STRATIS Investigators. Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke). Circulation. 2017;136:2311–2321. doi: 10.1161/CIRCULATIONAHA.117.028920. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
