

Urgent-Start Peritoneal Dialysis as a Bridge to Definitive Chronic Renal Replacement Therapy: Short- and Long-Term Outcomes
- PMID: 30662408
- PMCID: PMC6328466
- DOI: 10.3389/fphys.2018.01830
Urgent-Start Peritoneal Dialysis as a Bridge to Definitive Chronic Renal Replacement Therapy: Short- and Long-Term Outcomes
Abstract
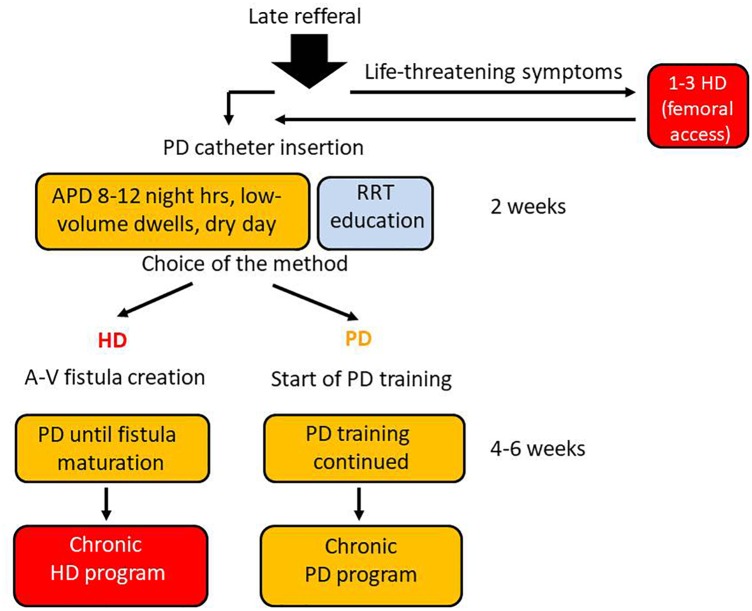
Background: The peritoneal dialysis (PD) urgent-start pathway, without typical 2-week break-in period, was meant for late-referral patients able and prone to join PD-first program, with its main advantages such as: keeping the vascular system intact, preserving their residual renal function and retaining life-style flexibility. We compared the short- and long-term outcomes of consecutive 35 patients after urgent- and 94 patients after the planned start of PD as the first choice. Methods: The study included all incident end-stage renal disease patients starting PD program between January 2005 and December 2015, classified into two groups: those with urgent (unplanned) and those with elective (planned) start. Urgent PD was initiated as an overnight automatic procedure (APD) with dwell volume gradually increased, and after 2-3 weeks, target PD method was established. Results: The mean time between catheter implantation and PD start was 3.5 ± 2.3 in urgent and 16.2 ± 1.7 days in planned-start groups (p < 0.00001). 51% of the patients in the urgent-start group required PD during first 48 h after catheter insertion. Mean follow-up of 17.6 ± 11.09 months (median: 19.0) was in the urgent-start group and 28.6 ± 26.6 months (median: 19.5) in the planned-start group. The early mechanical complications were observed more often in the urgent-start group (29 vs. 4%, p = 0.00005). The only significant predictors of early mechanical complications were serum albumin (p = 0.02) and time between the catheter insertion and PD start. The first year patient survival and technique survival censored for death and kidney transplantation were not significantly different between groups. In Cox proportional analysis the independent risk factors for patient survival as well as for method and patient survival appeared Charlson Comorbidity Index CCI (HR 1.4; p = 0.01 and 1.24; p = 0.02) and time from catheter implantation to PD start with HR 5.11; p = 0.03 and 4.29; p = 0.04 for <2 days, while time >14 days lost its predictive value (p = 0.07). Conclusion: Peritoneal dialysis may be a feasible and safe alternative to HD in patients who need to start dialysis urgently without established dialysis access, with an acceptable complications rates, as well as patient and technique survival.
Keywords: infectious complications; long-term outcomes; mechanical complication; patient survival; peritoneal dialysis; short-term outcomes; technique survival.
Figures
References
-
- Banli O., Altun H., Oztemel A. (2005). Early start of CAPD with the Seldinger technique. Perit. Dial. Int. 25 556–559. - PubMed
LinkOut - more resources
Full Text Sources