

Management of supracondylar fractures of the humerus in children
- PMID: 30662761
- PMCID: PMC6335593
- DOI: 10.1302/2058-5241.3.170049
Management of supracondylar fractures of the humerus in children
Abstract
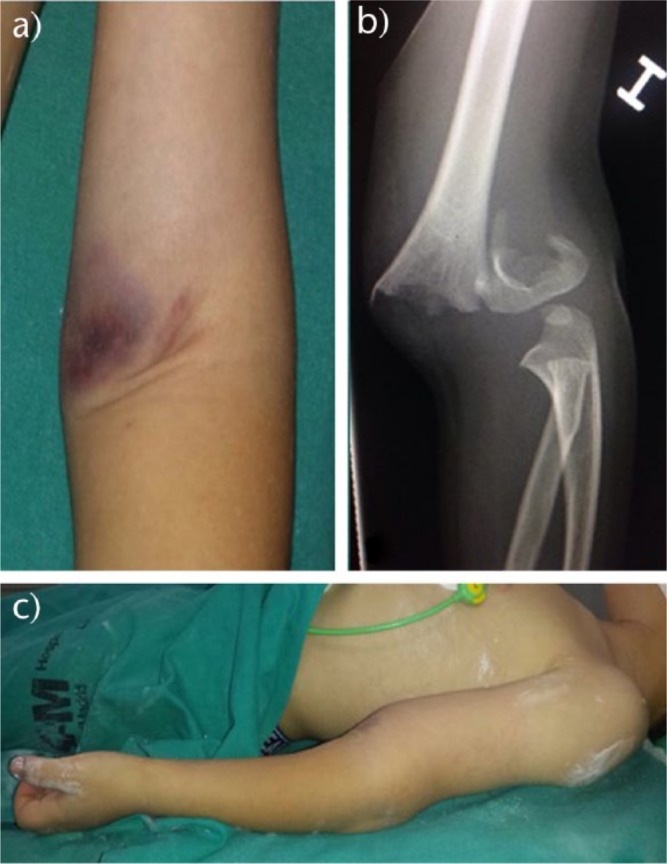
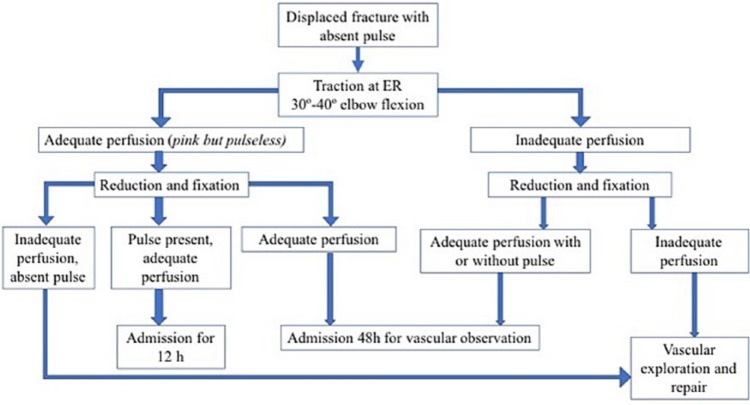
Supracondylar fractures of the humerus are the most frequent fractures of the paediatric elbow, with a peak incidence at the ages of five to eight years.Extension-type fractures represent 97% to 99% of cases. Posteromedial displacement of the distal fragment is the most frequent; however, the radial and median nerves are equally affected. Flexion-type fractures are more commonly associated with ulnar nerve injuries.Concomitant upper-limb fractures should always be excluded. To manage the vascular status, distal pulse and hand perfusion should be monitored. Compartment syndrome should always be borne in mind, especially when skin puckering, severe ecchymosis/swelling, vascular alterations or concomitant forearm fractures are present.Gartland's classification shows high intra- and inter-observer reliability. Type I is treated with casting. Surgical treatment is the standard for almost all displaced fractures. Type IV fractures can only be diagnosed intra-operatively.Closed reduction and percutaneous pinning is the gold standard surgical treatment. Open reduction via the anterior approach is indicated for open fractures, absence of the distal vascular flow for > 10 to 15 minutes after closed reduction, and failed closed reduction.Lateral entry pins provide stable fixation, avoiding the risk of iatrogenic ulnar nerve injury.About 10% to 20% of displaced supracondylar fractures present with alterations in vascular status. In most cases, fracture reduction restores perfusion.Neural injuries occur in 6.5% to 19% of cases involving displaced fractures. Most of them are neurapraxias and it is not routinely indicated to explore the nerve surgically. Cite this article: EFORT Open Rev 2018;3:526-540. DOI: 10.1302/2058-5241.3.170049.
Keywords: children; management; supracondylar fractures.
Conflict of interest statement
ICMJE Conflict of interest statement: None declared.
Figures






References
-
- Beaty JHKJ. Supracondylar fractures of the distal humerus. In: Beaty JH, Kasser JR, ed. Rockwood and Wilkins’ fractures in children. 6th ed. Philadelphia: Lippincott Williams and Wilkins; 2006:543-589.
-
- Omid R, Choi PD, Skaggs DL. Supracondylar humeral fractures in children. J Bone Joint Surg [Am] 2008;90-A(5):1121-1132. - PubMed
-
- Mulpuri K, Hosalkar H, Howard A. AAOS clinical practice guideline: the treatment of pediatric supracondylar humerus fractures. J Am Acad Orthop Surg 2012;20(5):328-330. - PubMed
-
- Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J Pediatr Orthop B 2001;10(1):63-67. - PubMed
-
- Moraleda L, Diez J, Valencia M. Is timing for paediatric supracondylar fractures related to pinning errors or complications? Podium presentation, POSNA Annual Meeting 2015, Atlanta, US.
LinkOut - more resources
Full Text Sources
Medical
