

Impact of Early versus Late Initiation of Renal Replacement Therapy in Patients with Cardiac Surgery-Associated Acute Kidney Injury: Meta-Analysis with Trial Sequential Analysis of Randomized Controlled Trials
- PMID: 30662912
- PMCID: PMC6312615
- DOI: 10.1155/2018/6942829
Impact of Early versus Late Initiation of Renal Replacement Therapy in Patients with Cardiac Surgery-Associated Acute Kidney Injury: Meta-Analysis with Trial Sequential Analysis of Randomized Controlled Trials
Abstract
Background: Previous studies have examined the effect of the initiation time of renal replacement therapy (RRT) in patients with cardiac surgery-associated acute kidney injury (CSA-AKI), but the findings remain controversial. The aim of this meta-analysis was to systematically and quantitatively compare the impact of early versus late initiation of RRT on the outcome of patients with CSA-AKI.
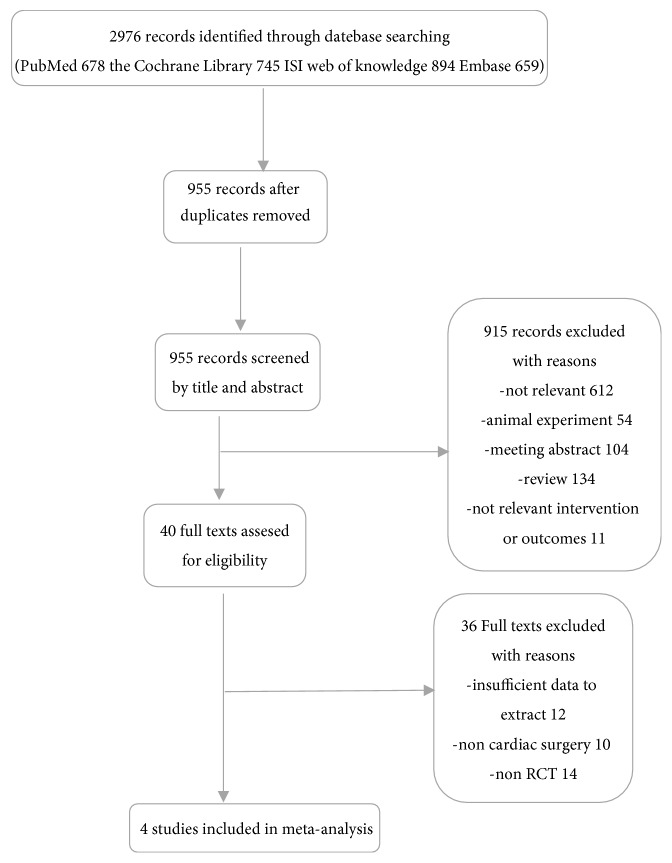
Methods: Four databases (PubMed, the Cochrane Library, ISI Web of Knowledge, and Embase) were systematically searched from inception to June 2018 for randomized clinical trials (RCTs). Two investigators independently performed the literature search, study selection, data extraction, and quality evaluation. Meta-analysis and trial sequential analysis (TSA) were used to examine the impact of RRT initiation time on all-cause mortality (primary outcome). The Grading of Recommendations Assessment Development and Evaluation (GRADE) was used to evaluate the level of evidence.
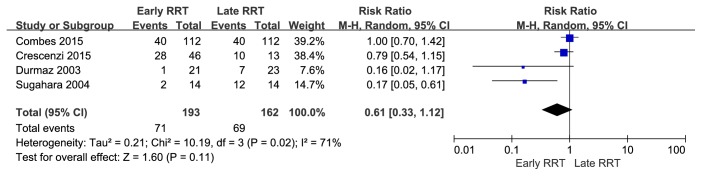
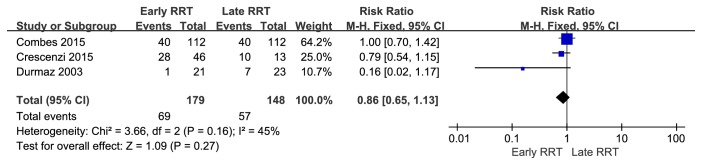
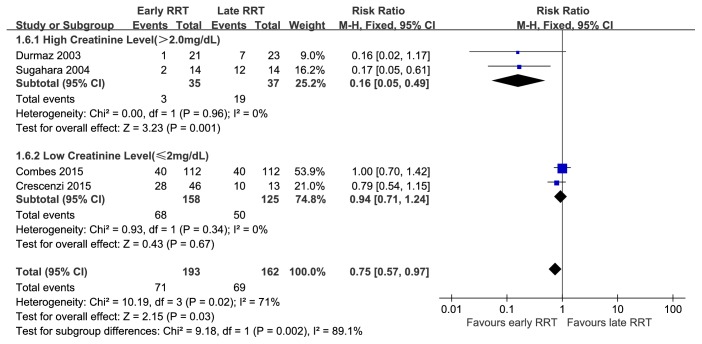
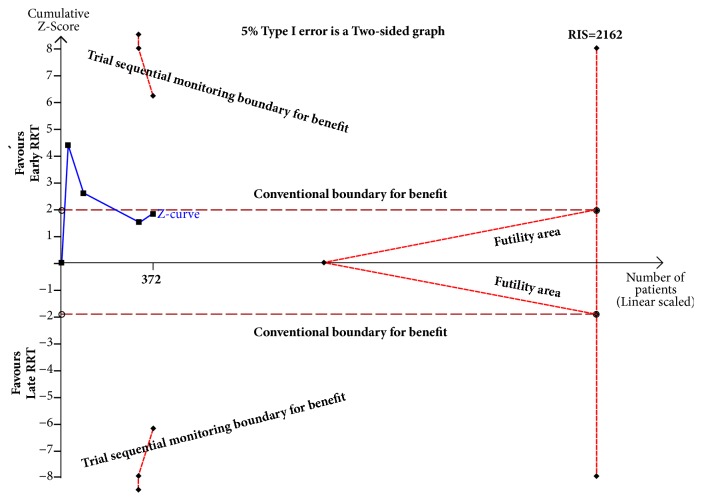
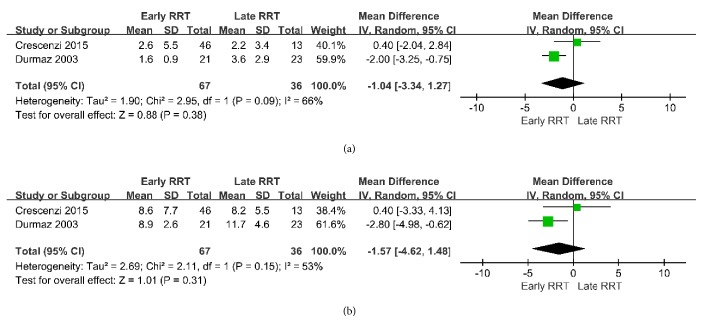
Results: We identified 4 RCTs with 355 patients that were eligible for inclusion. Pooled analyses indicated no difference in mortality for patients receiving early and late initiation of RRT (relative risk [RR] = 0.61, 95% confidence interval [CI] = 0.33 to 1.12). However, the results were not confirmed by TSA. Similarly, early RRT did not reduce the length of stay (LOS) in the intensive care unit (ICU) (mean difference [MD] = -1.04; 95% CI = -3.34 to 1.27) or the LOS in the hospital (MD = -1.57; 95% CI = -4.62 to 1.48). Analysis using GRADE indicated the certainty of the body of evidence was very low for a benefit from early initiation of RRT.
Conclusion: Early initiation of RRT had no beneficial impacts on outcomes in patients with CSA-AKI. Future larger and more adequately powered prospective RCTs are needed to verify the benefit of reduced mortality associated with early initiation of RRT.
Trial registration: This trial is registered with PROSPERO registration number CRD42018084465, registered on 11 February 2018.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
