

Patient safety, cost-effectiveness, and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults-study protocol for a stepped-wedge cluster randomized trial (PAWEL Study)
- PMID: 30665435
- PMCID: PMC6341754
- DOI: 10.1186/s13063-018-3148-8
Patient safety, cost-effectiveness, and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults-study protocol for a stepped-wedge cluster randomized trial (PAWEL Study)
Abstract
Background: Postoperative delirium is a common disorder in older adults that is associated with higher morbidity and mortality, prolonged cognitive impairment, development of dementia, higher institutionalization rates, and rising healthcare costs. The probability of delirium after surgery increases with patients' age, with pre-existing cognitive impairment, and with comorbidities, and its diagnosis and treatment is dependent on the knowledge of diagnostic criteria, risk factors, and treatment options of the medical staff. In this study, we will investigate whether a cross-sectoral and multimodal intervention for preventing delirium can reduce the prevalence of delirium and postoperative cognitive decline (POCD) in patients older than 70 years undergoing elective surgery. Additionally, we will analyze whether the intervention is cost-effective.
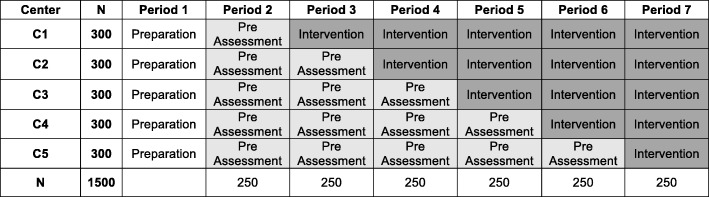
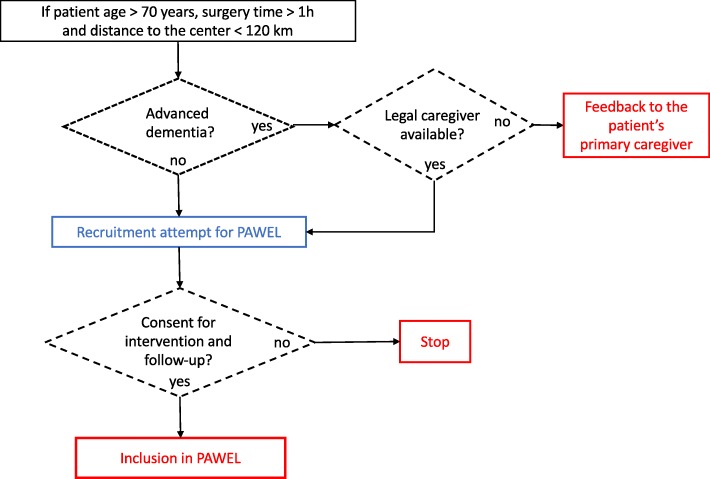
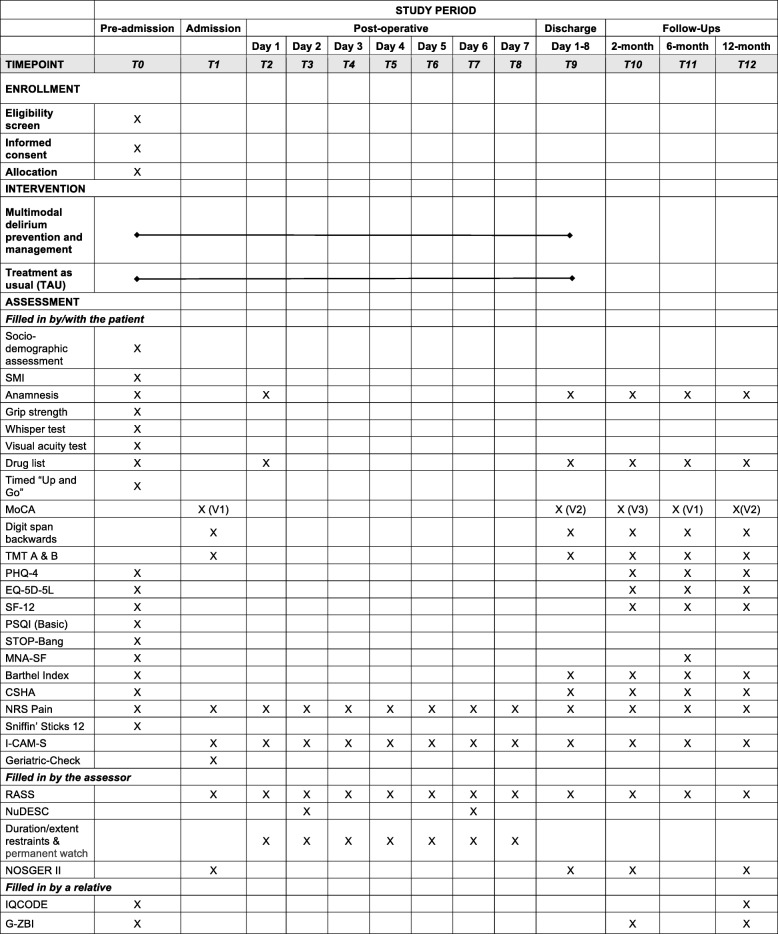
Methods: The study will be conducted at five medical centers (with two or three surgical departments each) in the southwest of Germany. The study employs a stepped-wedge design with cluster randomization of the medical centers. Measurements are performed at six consecutive points: preadmission, preoperative, and postoperative with daily delirium screening up to day 7 and POCD evaluations at 2, 6, and 12 months after surgery. Recruitment goals are to enroll 1500 patients older than 70 years undergoing elective operative procedures (cardiac, thoracic, vascular, proximal big joints and spine, genitourinary, gastrointestinal, and general elective surgery procedures).
Discussion: Results of the trial should form the basis of future standards for preventing delirium and POCD in surgical wards. Key aims are the improvement of patient safety and quality of life, as well as the reduction of the long-term risk of conversion to dementia. Furthermore, from an economic perspective, we expect benefits and decreased costs for hospitals, patients, and healthcare insurances.
Trial registration: German Clinical Trials Register, DRKS00013311 . Registered on 10 November 2017.
Keywords: Cost-effectiveness; Cross-sectoral care; Delirium prevention; Dementia; Elective surgery; Older patients; Postoperative cognitive dysfunction; Quality of life.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Ethics Commission of the Faculty of Medicine of the Eberhard-Karls University and University Hospital Tübingen with number 517/2017BO1 on October 12, 2017, and by the Ethics Commission of the University of Potsdam with number 38/2017 on December 11, 2017. The study was registered on the German Clinical Trials Register (number DRKS00013311,
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Witlox J, Eurelings LS, de Jonghe JF, Kalisvaart KJ, Eikelenboom P, Van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304(4):443–451. - PubMed
-
- Guenther U, Riedel L, Radtke FM. Patients prone for postoperative delirium: preoperative assessment, perioperative prophylaxis, postoperative treatment. Curr Opin Anaesthesiol. 2016;29(3):384–390. - PubMed
-
- Todd O, Gellrich L, Maclullich A, Driessen M, Thomas C, Kreisel S. Sleep disruption at home as an independent risk factor for postoperative delirium. JAGS J Am Geriatr Soc. 2017;65(5):949–957. - PubMed
-
- Patel J, Baldwin J, Bunting P, Laha S. The effect of a multicomponent multidisciplinary bundle of interventions on sleep and delirium in medical and surgical intensive care patients. Anaesthesia. 2014;69(6):540–549. - PubMed
